Victor V Rao MBBS, DMRD, RDMS (APCA)
The right upper quadrant ultrasound exam is perhaps one of the most common ultrasound exams performed by sonographers and clinicians.
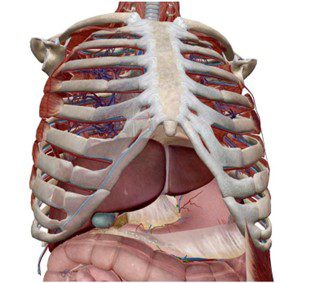
Fig. 1 Shows the anatomical relationships of structures in the right upper quadrant. The liver is the largest intraabdominal solid organ, as seen in the image.
Liver and gallbladder pathology is quite common, and interestingly a significant number of right upper quadrant scans are also reported as normal. Ultrasound is generally quite effective in ruling out the cause of pain in the right upper quadrant due to liver or gallbladder pathology. Findings such as liver mass, cysts, gallstones, and acute cholecystitis are commonly encountered.
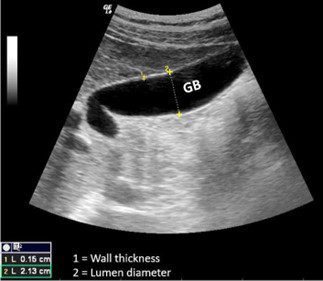
Fig. 2 A normal distended gallbladder with normal wall thickness.
The ideal transducer for performing an ultrasound exam of the liver and gallbladder is a low-frequency curvilinear transducer. The wide field of view is helpful to capture a large image. If a curvilinear transducer is unavailable, the phased array sector transducer may be used. When possible, scan with the patient in the supine position and examine the patient in the left lateral decubitus and upright position to avoid missing tiny gallstones.

Fig. 3 Shows a distended gallbladder with multiple gallstones. The gallstones are casting a clean acoustic shadow. The gallbladder wall is not thickened, and there is no evidence of fluid outside the gallbladder wall. This is a case of uncomplicated cholelithiasis.
In this article, we will briefly discuss acute cholecystitis and one potential life-threatening complication that may occur. Patients with acute calculous cholecystitis generally present with epigastric or right upper quadrant pain radiating to the right shoulder or scapula, nausea, vomiting, fever, and leukocytosis. Some patients may also have a known history of gallstones. Approximately 95% of cases of acute cholecystitis will have evidence of gallstone(s).
Ultrasound findings of acute cholecystitis may include:
- Gallbladder wall thickening
- Distended gallbladder
- Pericholecystic fluid (seen as an anechoic rim around the gallbladder)
- A positive sonographic Murphy sign
Sonographic Murphy sign and gallstones or evidence of a gallstone impacted in the neck of the gallbladder are the most sensitive ultrasound findings in acute cholecystitis.
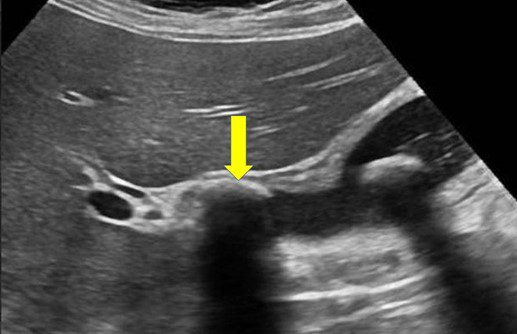
Image courtesy of UltrasoundCases.info owned by SonoSkills
Fig. 4 Shows stone-in-neck (SIN) sign positive—gallstone impacted in the neck of the gallbladder (yellow arrow). Another gallstone is seen within the lumen of the gallbladder, and the gallbladder wall is thickened. Sonographic Murphy sign was positive. A tiny rim of pericholecystic fluid is also visible. These results are consistent with acute cholecystitis.
Acute cholecystitis can be managed conservatively initially with antibiotics and intravenous fluids with a plan to perform an elective cholecystectomy after a few weeks. However, 2-30% of patients may develop gangrenous cholecystitis. This condition is life-threatening and is considered a surgical emergency. It must be verified on ultrasound.
Patients with gangrenous cholecystitis cannot be conservatively managed because there is necrosis of the gallbladder wall. Sonographic Murphy sign may be negative due to the necrosis of the gallbladder wall resulting in denervation of the gallbladder. Look for evidence of a hyperechoic intraluminal membrane-like structure within the gallbladder. Do not mistake it for an ultrasound artifact. The gallbladder wall may also be completely or partially disrupted with a collection of fluid and debris around the gallbladder.
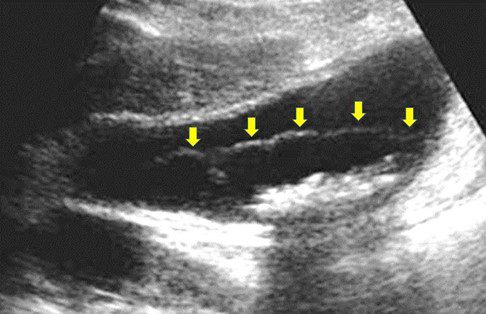
Fig. 5 Shows gangrenous cholecystitis. The gallbladder wall is thickened with an irregular echogenic membrane-like structure seen within the lumen of the gallbladder. Echogenic small gallstones are seen stacked together with an acoustic shadow in the dependent portion of the gallbladder. The sonographic Murphy sign was negative.
In conclusion, the physical exam alone is not sensitive enough to diagnose gangrenous cholecystitis. A negative Murphy sign on a physical exam could be seen in the absence of acute cholecystitis or in the presence of gangrenous cholecystitis. Point-of-care ultrasound (POCUS) must be used to rule out this potentially life-threatening condition. Other similar complications such as emphysematous cholecystitis may also develop with evidence of gas in the gallbladder wall and within the gallbladder lumen.
Ultrasound imaging will show echogenic reflectors within the gallbladder wall associated with a dirty shadow or ring-down artifact. The sonographic Murphy sign will be positive. Rarely we may see tiny echogenic foci rising within the bile in the gallbladder lumen. This is known as the champagne sign. Emphysematous cholecystitis has a higher risk of perforation of the gallbladder, and 50% of cases will not have any evidence of cholelithiasis.
The rapid adoption and use of POCUS by clinicians globally will help diagnose life-threatening complications of acute cholecystitis leading to immediate surgical intervention and lower mortality rates associated with these complications.
References
Adachi, T., Eguchi, S., Muto, Y. 2021, February 11. Pathophysiology and pathology of acute cholecystitis: A secondary publication of the Japanese version from 1992. Retrieved Apr 11, 2022, from DOI: 10.1002/jhbp.912.
Vadera, S. 2022, April 08. Acute cholecystitis. Retrieved April 11, 2022 https://radiopaedia.org/articles/acute-cholecystitis?lang=us.