Victor V Rao MBBS, DMRD, RDMS (APCA)
Point-of-care ultrasound (POCUS) can make a difference in managing patients suspected to have skin and soft tissue infections (SSTIs). SSTIs occur due to a breach of the skin or its supporting structure. SSTIs may have a wide array of clinical presentations. On a physical exam, SSTIs may present as cellulitis, an abscess, folliculitis, or vesicles. These conditions are usually identified during the physical exam.
At times we are presented with cases where we cannot determine if it is just cellulitis, an abscess, or a more complex picture of cellulitis with a coexisting abscess in some segments of the affected areas. It is important to differentiate between cellulitis and abscess because cellulitis can be managed effectively with broad-spectrum antibiotics and other supportive therapy. However, an abscess must be treated by incision followed by drainage or needle aspiration of pus in addition to antibiotics and other forms of treatment.
Let us briefly review the skin histology. The skin comprises a superficial epidermis and a deeper, thicker layer called the dermis. The hypodermis, also known as subcutaneous fascia, is the layer deep to the dermis. It is the deepest layer of skin, containing adipose tissue (fat) and subcutaneous connective tissue.
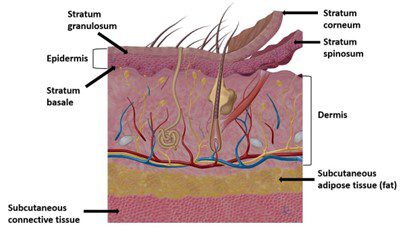
Figure: 1 Histology of skin and subcutaneous tissue
Normal Ultrasound of the Skin
Visualizing the very thin superficial epidermis, the slightly thicker dermis, and subcutaneous fat is possible using B-mode high-frequency ultrasound. A thin layer of echogenic fascia is seen deeper to the adipose tissue layer, followed by the muscle and bony tissue when present in that region, as seen in Figure 2. You may use a water bath, a thick layer of gel, or even an acoustic standoff pad during scanning to aid in improved image quality.
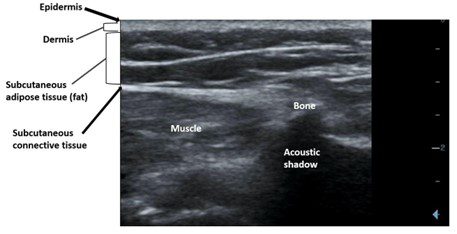
Figure 2: Normal ultrasound appearance of the skin, subcutaneous tissue, muscle, and bone
Cellulitis
In cellulitis, we will see the following ultrasound findings:
- Increased thickness of the dermis (compared with normal side)
- Hyperechoic subcutaneous tissue layer
- Evidence of edema/anechoic branching pattern (referred to as cobblestone pattern)
- Maintenance of tissue architecture
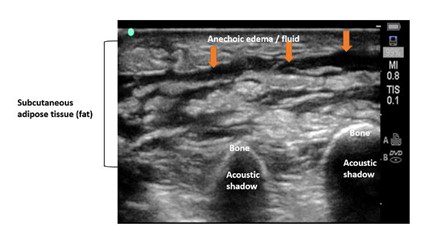
Figure 3: B-mode image shows cobblestone pattern. Subcutaneous adipose tissue appears hyperechoic with edema between fat lobules. The tissue architecture is maintained. No evidence of abscess is seen. Findings are consistent with cellulitis.

Figure 4: Cellulitis with a cobblestone pattern
Soft Tissue Abscess
The following ultrasound findings may be visible in a subcutaneous abscess:
- Irregular or ill-defined collection
- Disruption of normal architecture and appearance in the region with the abscess
- Evidence of echogenic debris, septation, or even gas bubbles
- A surrounding cobblestone pattern may still be seen if the surrounding tissue has evidence of cellulitis
- Collection may be anechoic, hypoechoic, or heterogeneous
- Compression with transducer may elicit movement of pus through the abscess
- Increased surrounding vascularity is seen on color Doppler or power Doppler
- Too much gas in the abscess may make it challenging to scan
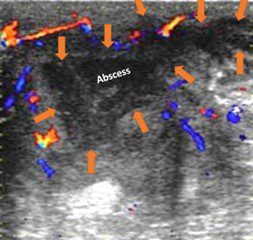
Figure 5: Ultrasound image of an SSTI using B-mode and color Doppler. An irregular hypoechoic collection is seen. Surrounding tissue shows increased vascularity. Note that the cobblestone appearance is not seen in the region of the abscess. Image courtesy of UltrasoundCases.info, owned by SonoSkills.
Often, we may be able to clinically diagnose an abscess by the presence of purulent discharge and obvious localized swelling and fluctuance. If the abscess size is small, there may be no need to do an incision and drainage. It could be treated with needle aspiration under ultrasound guidance. Scan with color Doppler or power Doppler to identify any major vessel or important structure in the region to avoid vascular injury, hemorrhage, or other serious injury during the procedure.
Interested in learning more about POCUS Musculoskeletal Soft Tissue assessment? Explore our library of educational resources to access a wealth of tools to support your own development.
Access the full POCUS Learning Library for FREE!
Share a few details so we can tailor new content to your specialty and region.



















