Back to COVID-19 Main Page
By Victor V Rao MBBS, DMRD, RDMS
Statement Update April 20, 2020
The role of point-of-care ultrasound (POCUS) lung has been established, and the lung ultrasound findings in COVID-19 patients seem consistent with a viral pneumonia pattern. Some patients develop a more severe disease presentation that mimics ARDS.
Newer data reported also brought to light cardiac issues that were not reported during the earlier stages of the coronavirus pandemic.
The transducer of choice for a focused cardiac exam would be a low frequency phased array transducer.
Here are some of the recommended views:
- Parasternal long-axis view (PLAX) including the descending thoracic aorta
- Parasternal short-axis view (PSAX) – mid ventricle and apical
- Apical 4 chamber view (A4C – B-mode and color Doppler)
- Apical 3 chamber view
Some significant echocardiographic findings that could be seen in COVID-19 patients with cardiac involvement are:
- Increased wall thickness with diffuse biventricular hypokinesis, especially in the apical segments
- Severe left ventricular dysfunction with reduced EF
- Right heart failure
- Biventricular myocardial interstitial edema
- Pericardial effusion – most notable around the right cardiac chambers
- Some patients also develop myocardial infarction as the preexisting plaques in the coronary arteries become unstable due to inflammation. These would show reduced contractility of the heart with reduced EF and increased EPSS.
- Isolated reports of pulmonary embolism (PE) with dilated right ventricle and hyperdynamic apex of the RV and flattened septum with d-shaped LV
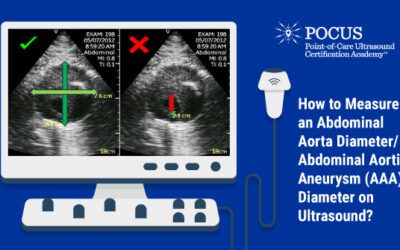
In conclusion, it is a good idea to evaluate the heart at the time of admission or triage with some basic views like PLAX, PSAX (mid ventricle), A4C, and others. This imaging is beneficial to have in case the patient does develop cardiac complications such as left or right heart failure, myocarditis or myocardial infarction, etc. It will help establish if cardiac complications were a result of COVID-19 or worsening of preexisting cardiac pathology.
Moderate to severe cardiac complications would need a consultation by a cardiologist in the near term, and additional follow up after recovery from the COVID-19 infection as there could be long-term cardiac complications.
March 20, 2020
For decades, there has been a concern amongst the medical community about potentially lethal viral diseases continuing to emerge in the human population. In 2002 there was the severe acute respiratory syndrome coronavirus (SARS – CoV), followed by H1N1 influenza in 2009 and the Middle East respiratory syndrome coronavirus (MERS-CoV) in 2012. In December 2019 and continuing to spread in 2020 we have the ongoing coronavirus (COVID-19) pandemic which has infected 191,127 individuals1 (confirmed cases) worldwide and has resulted in 7,807 deaths1 as of March 18, 2020. This new virus seems to be very contagious and has quickly spread globally and spared only a few countries in just 4 months as seen in the map below.

World map showing confirmed COVID-19 cases (shaded areas) as of March 18, 2020 2
Imaging for COVID-19
The following modes of radiological imaging tools may be used.
- Chest X-ray – abnormal in 60-77%.
- CT Scan (Chest) – abnormal in 86-95%.
- Point of Care Ultrasound (POCUS-Lung)
- Basic POCUS echocardiography to look for evidence of heart failure or myocarditis
The most common findings were bilateral with ground glass appearance, patchy consolidation, peripheral distribution, cystic changes, and mild effusions. Surprisingly the effusions were seen in less than 10% cases. Unilateral findings can be expected in early disease. POCUS lung ultrasound is not confirmatory of COVID-19 infection, but it can suggest the possibility of the COVID-19 infection in a patient and is also very helpful to monitor the progress of the disease in a patient.
POCUS Lung Findings for COVID-19
- Thickening of the pleural line with irregular pleural
- B-lines in a variety of patterns including focal, multifocal, and
- Consolidations in a variety of patterns including multifocal small, and lobar with occasional dynamic air
- Reappearance of A-lines during recovery
- Pleural effusions are uncommon but small effusions may be
- Positive ultrasound findings were seen more commonly in the basal region and the posterior chest.
- Lung sliding is seen in regions exhibiting A-lines and B-lines.
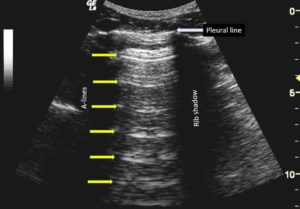
Figure showing B-mode ultrasound image of the normal chest with normal A-lines seen.
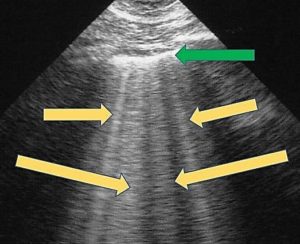
Figure showing B-lines (yellow arrows) and thickened pleura (green arrow) which can be seen in patients with COVID-19 chest involvement. Keep in mind that these findings are not specific to COVID-19. However, a return to normal A-line profile from the B-line profile would suggest that the patient may be improving.
Transducer Choice and Scanning Tips for COVID-19
POCUS Lung/Chest Ultrasound for COVID-19
Since B-lines are the common findings, we recommend using a low frequency curvilinear transducer with a “Lung” preset. If a curvilinear transducer is not available, then you can use a phased array low frequency transducer or even a linear transducer. The ideal depth would be about 15 cm on average to be able to visualize the A-lines and the B-lines effectively.
To visualize the pleural, we recommend depth settings of 5-7 cm with a lung preset. For this scan, you could also use a high frequency linear transducer.
Make sure to optimize the gain. Decreasing the gain may help with visualization. Scan with the transducer orientation marker in the cephalad direction. Check all chest zones and do not forget to scan the basal region of both lungs and the posterior chest.
Basic POCUS Echo for COVID-19
Use a low frequency phased array transducer with a frequency range of 2.0 to 5.0 MHz to image the heart. Obtain a left parasternal long axis view and an apical 4 chamber view. You may obtain additional cardiac views as well. Look for evidence of myocarditis or heart failure. Observe contractility and compare left and the heart and note any dilatation of cardiac chambers.
Transducer/US Equipment Disinfection for COVID-19
Make sure to follow proper disinfection procedures after scanning a COVID-19 infected patient. Follow the same for any patient who is suspected of having COVID-19 infection. While scanning the patient, it would be advisable to use a transducer cover or sheath to cover the transducer. If a transducer cover is not available, you could also use a glove. Make sure to put ultrasound coupling gel on the transducer head before covering it with an appropriate cover. Discard used probe cover applying the recommended methods.
An app based or any ultrasound device without any cooling fans would be a better choice as the device can be adequately cleaned and disinfected after use.
COVID-19 presents a unique challenge to the healthcare community around the world. POCUS can play a vital role to triage and monitor patients who may be suspected of having the infection. Radiologists have recommended the use of bedside ultrasound/POCUS for diagnosing patients suspected to have the COVID-19 infection4.
References
- https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200318-sitrep-58-covid-19.pdf?sfvrsn=20876712_2
- https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/world-map.html
- https://link.springer.com/article/10.1007/s00134-020-05996-6
- https://www.radiologybusiness.com/topics/care-delivery/radiologists-ultrasound-covid-19-chest-x-ray-coronavirus
- https://jamanetwork.com/journals/jamacardiology/fullarticle/2763844
- https://newsnetwork.mayoclinic.org/discussion/how-does-covid-19-affect-the-heart/
- https://khn.org/news/mysterious-heart-damage-not-just-lung-troubles-befalling-covid-19-patients/
- https://www.heart.org/en/coronavirus/coronavirus-covid-19-resources
Looking for additional inspiration? Sign up for our POCUS Post™ newsletter to receive monthly tips and ideas.