By Victor Rao MBBS, DMRD, RDMS
Introduction
The inferior vena cava (IVC) is the largest vein of the body. It is located along the right anterolateral aspect of the vertebral column and brings deoxygenated blood from the lower extremities and abdomen to the right atrium. It runs posterior to the liver and becomes intrahepatic before connecting to the right atrium.
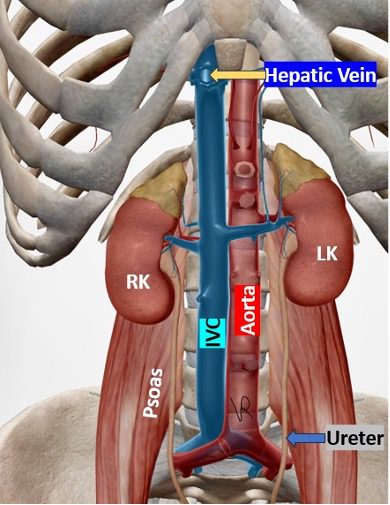
Figure 1. Observe location of the IVC (blue), abdominal aorta (red) and the hepatic veins draining into the IVC.
If you scan the subxiphoid region in the transverse plane, the abdominal aorta is seen towards the left side of the body. In comparison to the abdominal aorta, the IVC has thin walls and tends to collapse with respiration in a normal patient. In contrast the abdominal aorta is thick walled and does not vary with respiration and does show pulsatility with the cardiac cycle.
![]()
Figure 2. Transverse view at the level of the pancreas showing abdominal aorta (red) on the left side of the patient and the IVC (blue) towards the right side of the patient.
Ultrasound is an excellent non-invasive bedside tool for assessing the IVC which could be correlated with volume status and help guide fluid management, particularly in critical care and emergency settings. Be aware that in complex hemodynamic scenarios, IVC alone may not be able to provide a clear picture of fluid status and hemodynamics and may need to be correlated clinically and with more comprehensive fluid assessment bedside POCUS tools such as the VExUS protocol.
Transducer
I prefer to use a low-frequency curvilinear (3.0–5.5 MHz) or phased array probe (2–5 MHz) for IVC assessment with the former being my transducer of choice. If you are using a multifrequency transducer, make sure to select the abdomen setting for optimal imaging.
Patient positioning
The patient should be in a supine position with slightly flexed knees. Flexing the knees helps to relax anterior abdominal muscles. If the anterior abdominal wall is not rigid, you may have the patient keep the legs straight.
Views and measurements
Subcostal long-axis
Place the ultrasound transducer in the subxiphoid region slightly to the right side of the patient’s midline with the transducer image orientation marker pointing cephalad (towards the patient’s head). Obtain a mid-long axis view of the IVC. Measure IVC diameter 1–2 cm distal to the hepatic vein–IVC junction during expiration (IVCmax) and inspiration (IVCmin). You may use M-mode to capture M-mode tracing to document and measure IVC variability with respiration. This is my preferred method as everything can be captured and measured in a single image as shown below.
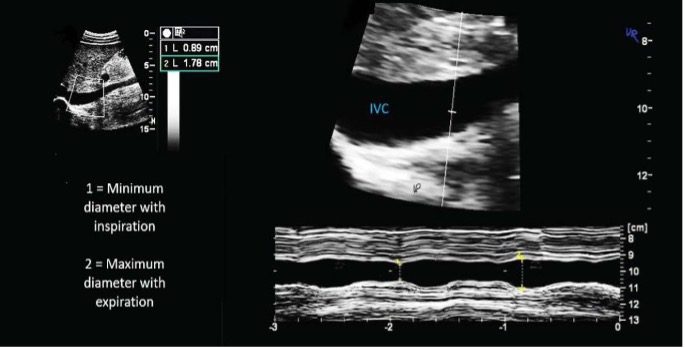
Figure 3. M-mode tracing on the IVC variation with normal respiration.

Figure 4. Location of transducer (yellow) in the subxiphoid region with the probe marker pointing cephalad and slightly to the right of the midline.
Right upper quadrant (RUQ)
This may be an alternative approach in pregnancy or challenging anatomy, using a mid-axillary coronal view. It is not an ideal view but could be used if you are unable to scan the IVC in the subxiphoid region.
Dynamic assessment
Calculate collapsibility index (cIVC) using the formula –
cIVC=IVCmax−IVCmin / IVCmax × 100%
| Mean RAP (mm Hg) | IVC Diameter (cm) | IVC Collapse (%) |
| 0-5 | <1.5 | >50 or total collapse |
| 6-10 | 1.5-2.5 | >50% |
| 11-15 | 1.5-2.5 | <50% |
| 16-20 | >2.5 | <50% |
| >20 | >2.5 | >No change |
Table 1. Spontaneous breathing (not holding breath, or mechanically ventilated). Corresponding approximate right atrial pressure (RAP).
Clinical Applications
Hypovolemia
Small or collapsed IVC (<1.5 cm) with >50% collapse.
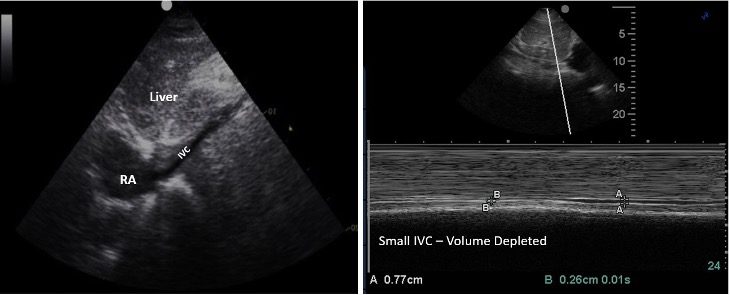
Figure 5. The image on the left shows mid-longitudinal view of the IVC draining into the right atrium. M-mode tracing shows IVC maximum diameter of 0.77 cm and a minimum diameter of 0.26 cm. This patient was hypovolemic and benefitted from intravenous fluid replacement.
Volume overload
Plethoric IVC (>2.5 cm) with minimal respiratory variation. <20% indicates volume overload. Some exceptions may apply. Always correlate clinically. It should fit the clinical picture.
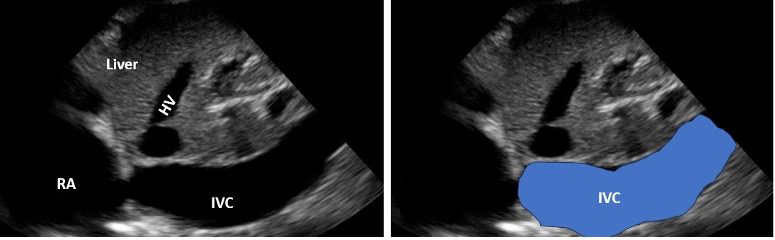
Figure 6. Large plethoric IVC. The IVC diameter did not vary with respiration or sniffing. Be aware that in some super athletes the IVC could appear dilated due to the large venous reserve. However, the IVC diameter will vary by 50% or more with respiration or sniffing in normal athletic individuals.
Heart failure management
IVC assessment can be used to guide decongestion therapy in acute decompensated cases.
Limitations and Considerations
Confounding factors
Elevated intra-abdominal pressure, mechanical ventilation, and right heart failure can alter IVC hemodynamics.
Pregnancy
RUQ window provides better image quality than subcostal approach. Keep in mind that since it is an oblique view of the IVC, the eyeball observation should be used to get a general idea. Think about extreme situation such as a collapsed IVC versus a plethoric IVC with no change with respiration.
Pitfalls
Differentiate IVC from aorta. The simple table below may help you differentiate IVC from abdominal aorta. Review Figure 1 also.
| Feature/Observation | IVC | Abdominal Aorta |
| Side of patient | Right side | Left side |
| Transverse view cross section | Elliptical | Circular |
| Wall thickness | Thick | Thin |
| Variation with respiration (normal) | Yes | No |
| Variation with sniffing (normal) | Yes | No |
| Spectral Doppler waveform | Venous waveform | Arterial waveform |
| Right renal artery passes under in long view |
Yes | No |
| Branches such as celiac artery and SMA | No | Yes |
| Drains into the right atrium | Yes | No |
Table 2. Comparison of IVC and abdominal aorta on ultrasound.
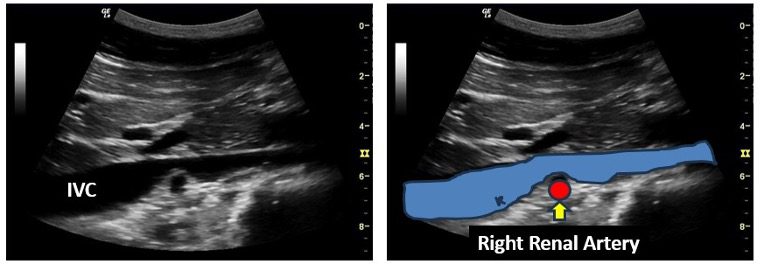
Figure 7. IVC – mid longitudinal view. Observe the right renal artery passing posterior to the IVC.
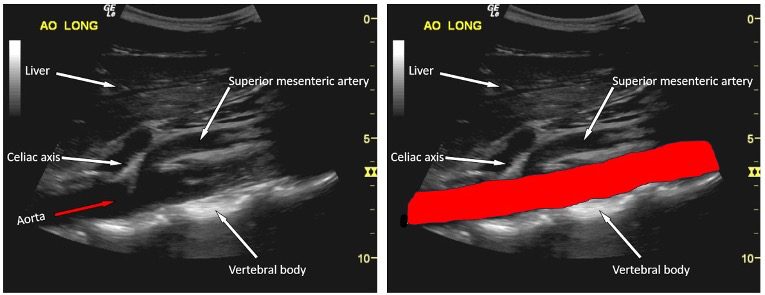
Figure 8. Mid-longitudinal view of the abdominal aorta (red) at the level of upper and mid abdominal aorta. Observe how different it is as compared to the IVC.
There may be some factors that may make imaging the IVC challenging using ultrasound. These factors could be divided into subgroups such as thoracic (chest), abdominal or both. Please see the table below.
| Thoracic |
| Emphysema |
| Pneumothorax |
| Abdominal Factors/Conditions |
| IVC occlusion due to thrombus |
| Advanced stage fatty liver |
| Ascites |
| Bowel gas |
| Pneumoperitoneum |
| Guarding and rigidity due to pain |
| Combined Thoracic and Abdominal Factors |
| Surgical scar |
| Open wound or incision in the subxiphoid region |
| Subcutaneous emphysema |
| Obesity |
Table 3. Various factors that may make imaging the IVC using ultrasound difficult or challenging.
Conclusion
The IVC collapsibility index shows 78% sensitivity and 86% specificity for fluid responsiveness. IVC assessment along with lung ultrasound improves accuracy in distinguishing intravascular versus extravascular volume overload. Multiple peer-reviewed studies have validated its utility in diverse settings, including sepsis, dialysis, and perioperative care. Always correlate findings in the clinical context and multiorgan POCUS assessments (e.g., cardiac function, lung ultrasound etc.) must be considered. Get familiar with VExUS protocol for more complex hemodynamic situation assessment.
References
Access the full POCUS Learning Library for FREE!
Share a few details so we can tailor new content to your specialty and region.



















