By Victor V Rao MBBS, DMRD, RDMS
Introduction
Renal colic is commonly characterized by acute, severe flank pain. It is frequently caused by ureteral stones obstructing urinary flow. The diagnostic gold standard is non-contrast CT. It offers high accuracy but has high cost, risks of ionizing radiation exposure, and resource implications. Recent years have seen the rise of point-of-care ultrasound (POCUS) as an effective, non-invasive tool in the assessment of suspected renal colic.
Why Use POCUS for Renal Colic
POCUS presents several advantages:
- Rapid assessment
- Immediate availability at the point of care providing timely care and diagnosis
- No ionizing radiation
- Low cost
- Reproducible and easy to perform follow up scans
- Improved patient care
- Can potentially decrease emergency department length of stay
Transducer Selection
Ideal transducer for this application is a low frequency curvilinear transducer. You may also use a low frequency phased array transducer if the curvilinear transducer is not available. Modern multifrequency transducer with a broad frequency range may also be used if the frequency in the range of 3.0 to 5.0 MHz is available.
Preset
Use renal or abdomen preset. For the longitudinal view, scan with the transducer orientation marker pointing cephalad. For a transverse view, scan with the transducer orientation marker pointing to the patient’s right side. Using the renal preset may allow some specific inbuilt calculation packages for urinary system evaluation. For example – bladder volume calculation using the ultrasound device.
Patient Position
The ideal patient position is supine. Additional views can be obtained in the left and right lateral decubitus positions. Sometimes, we may even consider the prone position to scan from the back if the above-mentioned positions do not yield optimal view of the kidneys.
Normal Ultrasound Findings
Right Kidney
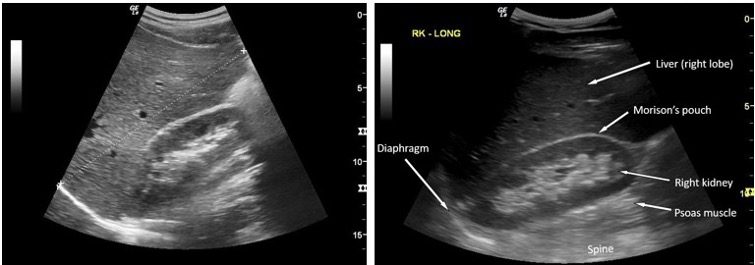
Figure 1. Longitudinal view of the right kidney. Observe the echogenic normal pelvicalyceal system. There is no evidence of hydronephrosis, or calculi seen.
Left Kidney
The view of the left kidney may sometimes be more challenging to obtain due to bowel gas in the splenic flexure of the colon obstructing the view. Scan with the patient in the supine or right lateral decubitus position. Position the transducer in the right lower intercostal region in the left posterior axillary line with the ultrasound beam aimed towards the left kidney.
Ureters
The ureters are generally not visible if there is no obstruction to flow of urine from the renal pelvis to the bladder. In some cases, bladder outlet obstruction due to advanced stage of BPH may cause backpressure to distend the ureters. Common scenario would be an obstruction to the flow of urine due to a ureteric calculus. Ureteric calculus may be challenging to diagnose for the new user. Lower ureteric calculus obstructed at the uretero-vesical junction may be easier to image with ultrasound. Simply follow the ureter from the pelvi-ureteric junction down when the ureter is distended.
Bladder
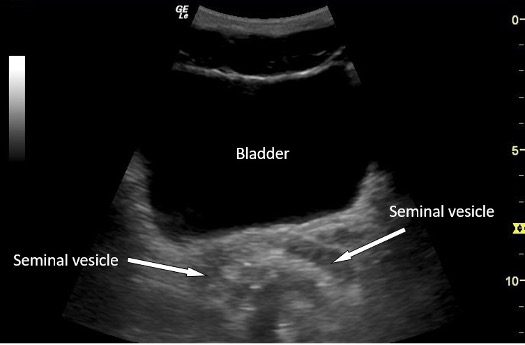
Figure 2. Transverse view of the bladder in a male patient. This is a normal bladder view with no calculus, debris or mass seen with the bladder lumen.
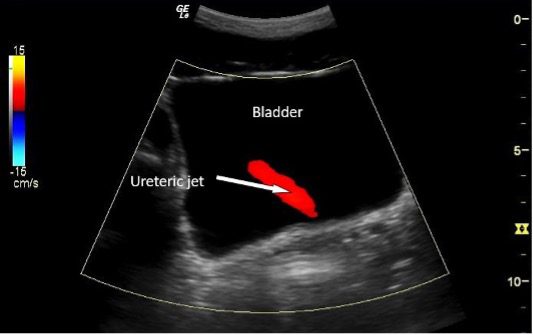
Figure 3. Ureteric jet demonstrated using color Doppler. There should be 1-3 ureteric jets observed in a normal well-hydrated patient with no ureteric obstruction.
Diagnostic Findings With POCUS
Hydronephrosis
The primary role of POCUS in renal colic is the detection of hydronephrosis (dilation of the renal pelvis and calyces due to urinary obstruction).
Ultrasound Sensitivity – Ranges from 72–76% for hydronephrosis when performed by emergency medicine physicians.
Ultrasound Specificity – Ranges between 55–60%, improving for larger stones (>5mm).
Moderate or severe hydronephrosis strongly suggests obstruction secondary to urolithiasis. Be aware that the compression on the ureter could be also due to a mass or enlarged lymph node or even bladder outlet obstruction (those patients would not present with renal colic).
Direct Calculus Visualization
Even though ultrasound is less sensitive than CT scan, it may still help to image and diagnose calculi in most patients. The key findings are:
- Hyperechoic (bright), round, oval or irregular lesion (calculi) in the renal collecting system or ureter
- Calculi with posterior acoustic shadowing
- Twinkling artifact on color Doppler, very helpful to detect small calculi
Let us look at some examples below.
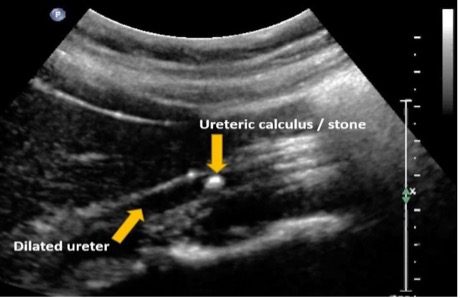
Figure 4. Single hyperechoic calculus in the ureter with proximal dilatation of the ureter (hydroureter).
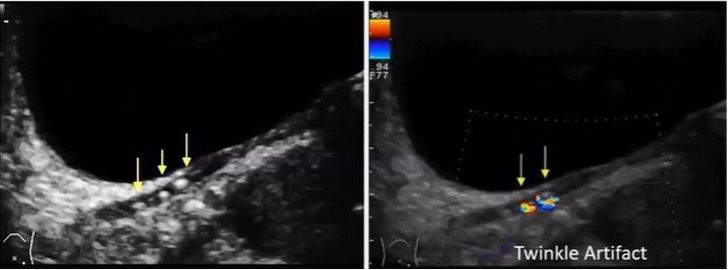
Figure 5. The image on the left shows hyperechoic calculi in the lower ureter. The calculi do not show any posterior acoustic shadowing because they are small. Renal calculi smaller than 3-5 mm (approximately) in diameter may not display posterior acoustic shadow. The image on the right shows twinkling artifacts. Images courtesy of ultrasoundcases.info
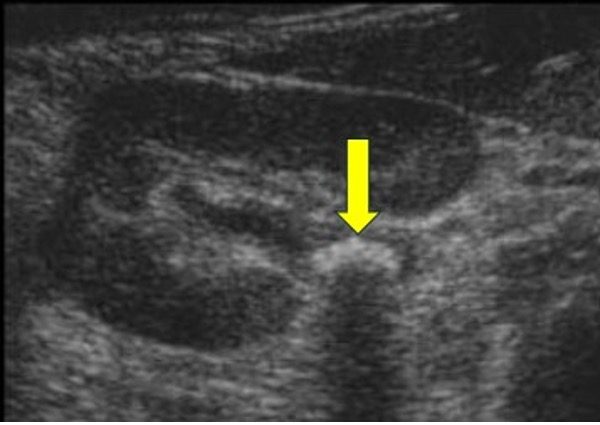
Figure 6. Transverse view of the kidney. Single, well defined echogenic calculus (yellow arrow) seen in the renal pelvis with a posterior acoustic shadow. Image courtesy of ultrasoundcases.info
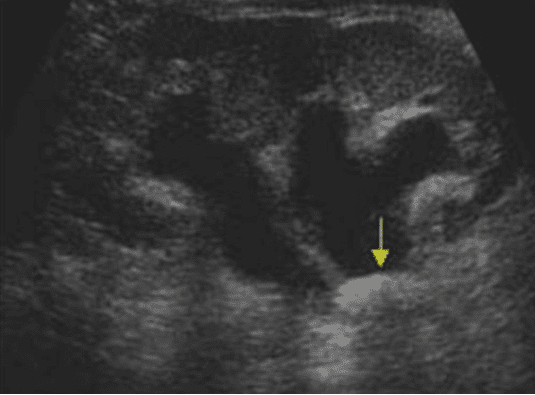
Figure 7. Longitudinal view of the kidney with moderate hydronephrosis. The renal calculus is located at the pelvi-ureteric junction. Image courtesy of ultrasoundcases.info
Assessing Complications
POCUS can also be used to detect complications such as pyelonephritis, perinephric fluid/urinoma suggesting forniceal rupture. See images below.
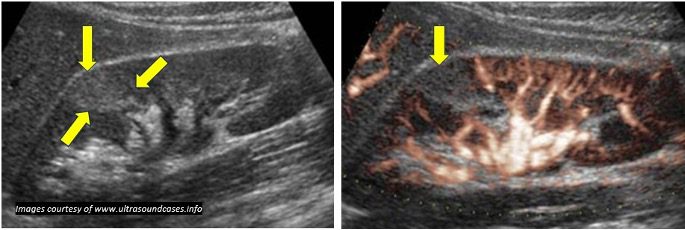
Figure 8. The B-mode image on the left shows a suspicious hyperechoic lesion. The eFlow image on the right shows evidence of diminished vascularity in the suspicious region. Findings and clinical history and other lab results were consistent with pyelonephritis. eFlow is a high-definition blood flow imaging mode and may be available only in some advanced ultrasound devices.
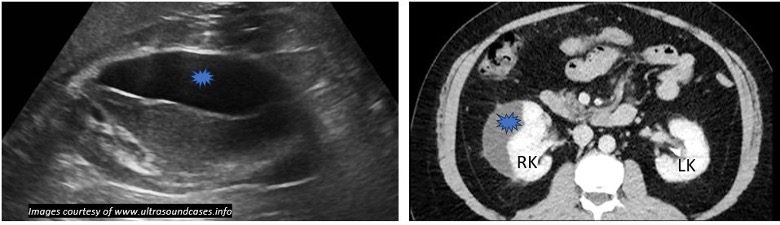
Figure 9. The ultrasound image on the left shows an anechoic collection outside the right kidney which was reported as a urinoma. The image on the right shows a CT scan image showing the same lesion (blue). Always correlate clinically.
Role of CT scan
In high-risk individuals who continue to have fever or individuals with a one functioning kidney, transplant history or suspected infection CT scan may be indicated to make a definitive diagnosis.
Clinical Workflow
- Initial Assessment – History, exam, urinalysis.
- POCUS – Identify hydronephrosis and, if possible, stone.
- Management – If mild/no hydronephrosis, normal ureteric jet observed on the affected side, good pain control, low-risk features – outpatient management. If moderate/severe hydronephrosis or failure to improve consider CT and/or urology referral. Educate the patient about the risk of kidney damage if left untreated.
CT scan
If an ultrasound examination is inconclusive due to bowel gas or a patient’s body habitus, then CT scan should be considered if there is concern about moderate or severe hydronephrosis
Evidence and Guidelines
Guidelines recommend considering ultrasound as the initial imaging in typical, low-risk presentations.
Some commonly encountered Scenarios in Renal Colic patients
- Renal Calculus with acoustic shadow – A bright (hyperechoic) lesion in the lower calyx, with a dark posterior shadow, is characteristic of a renal stone. See figure 14.
- Hydronephrosis – Dilated renal pelvis and calyces indicating obstruction—graded as mild, moderate, or severe.

Figure 10. Mild hydronephrosis
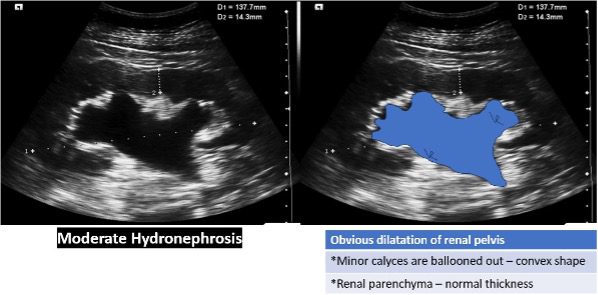
Figure 11. Moderate hydronephrosis
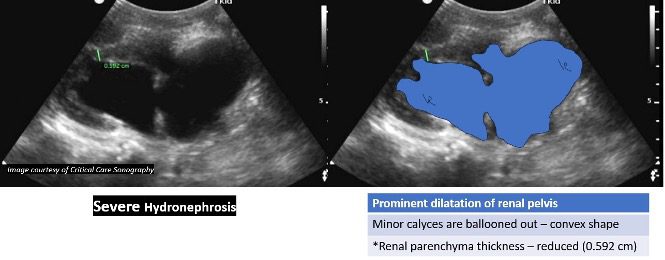
Figure 12. Severe hydronephrosis. In this case the renal parenchyma thickness is 0.592 cm. Normal thickness is 1.5 cm.
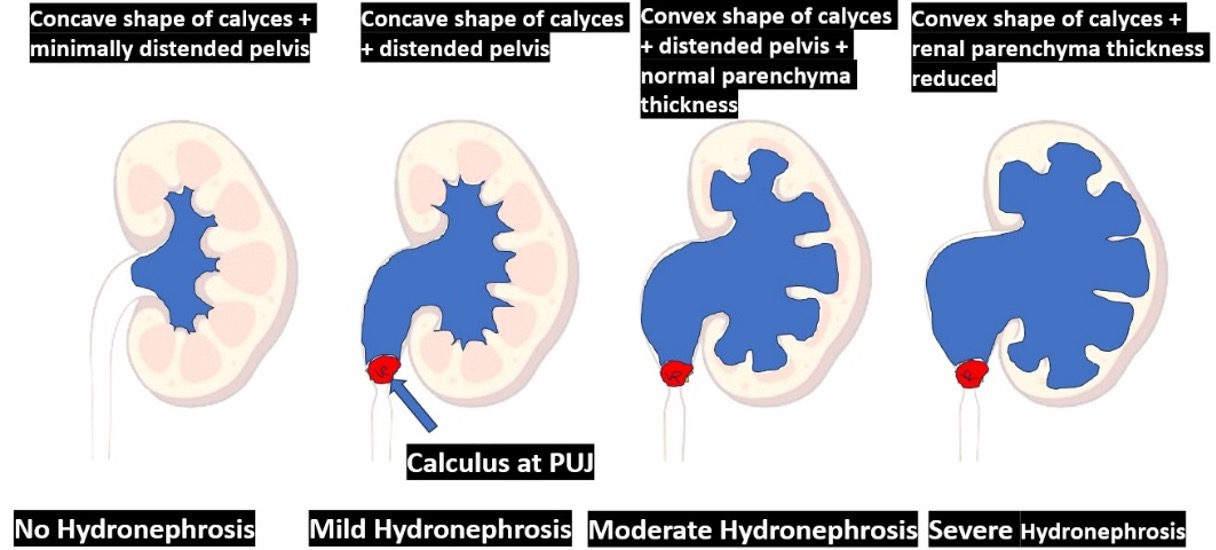
Figure 13. Diagrammatic representation of different grades of hydronephrosis. It is important to note that in severe hydronephrosis there is a significant reduction in renal parenchyma thickness. In chronic cases with severe hydronephrosis, the renal parenchyma may be destroyed, and the kidney may appear like a giant anechoic cyst.
Doppler Twinkling Artifact
Color Doppler showing the “twinkling artifact” posterior to a stone can aid in detection and confirmation of renal calculi especially small calculi.
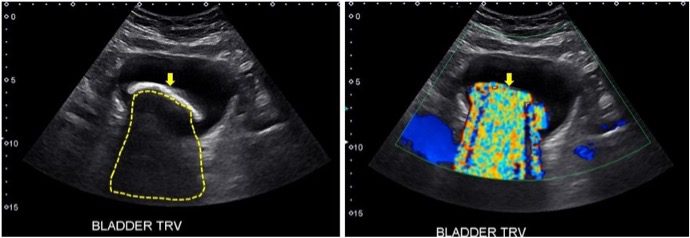
Figure 14. The image on the left shows a B-mode transverse image of the bladder with a large echogenic calculus within the lumen of the bladder. There is a dense acoustic shadow seen posterior to the calculus. The image on the right shows twinkling artifact posterior to the calculus during color Doppler mode. This is confirmatory that it is a calculus. In this case it was very clear there is a large calculus seen in B-mode imaging. The twinkling artifact is useful to confirm small renal calculi. Images courtesy of renalfellow.org
Conclusion
POCUS is an excellent tool for the evaluation of a patient with suspected renal colic. It allows for rapid evaluation of the urinary system to look for evidence of renal calculi and/or hydronephrosis. It may help reduce unnecessary CT scan use and improve patient care and resource utilization.
CT scans may still be required in individuals with a high BMI or non-visualization of the urinary system with ultrasound due to technical reasons. We can reduce unnecessary ionizing radiation exposure to the patients by embracing an “ultrasound-first” approach paired with proper relevant history, physical examination in addition to POCUS findings to improve patient safety and quality of care.
References



















