By Kamal Alao Ashimiyu
Introduction
Point-of-care ultrasound (POCUS) is increasingly recognized as an essential examination in the bedside evaluation of hepatobiliary disorders. Its application in diagnosing biliary colic and acute cholecystitis has proven valuable due to its accessibility, rapid diagnostic accuracy. In this blog, I examine the role of POCUS in diagnosing these conditions, highlighting its advantages, limitations, and practical applications. Biliary colic and acute cholecystitis are common causes of right upper quadrant (RUQ) pain in most patients having complications related to the abdomen, it is therefore very important to have a quick diagnosis to prevent complications such as sepsis, gallbladder perforation, or peritonitis (1,2).
Pathophysiology of Biliary Pathology
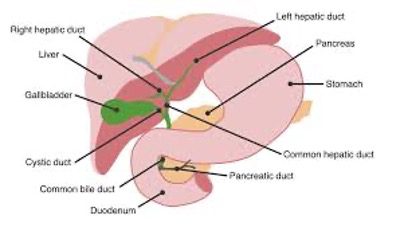
Figure 1. Diagrammatic representation of the liver, biliary tree and gallbladder and other structures in the vicinity.
Biliary Colic
Biliary colic occurs due to transient obstruction of the cystic or common bile duct by gallstones. Patients typically present with periodic RUQ pain radiating to the shoulder, often following fatty meals. The absence of significant inflammation differentiates biliary colic from acute cholecystitis (3).
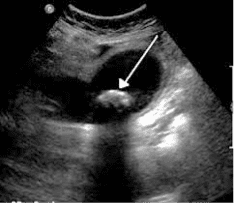

Figure 2. The upper image shows a large echogenic gallstone in the lumen of the gallbladder. The gallbladder wall appears to be slightly thickened. The calculus is not impacted in the neck of the gallbladder. No pericholecystic fluid seen. Observe the posterior acoustic shadow. The lower image shows multiple gallstones. One stone appears to be impacted in the region of the neck of the gallbladder. The gallbladder wall is markedly thickened with a small amount of anechoic pericholecystic fluid. This is consistent with acute calculus cholecystitis.
Acute Cholecystitis
Acute cholecystitis, on the other hand, involves prolonged cystic duct obstruction leading to gallbladder wall inflammation. Clinical signs include persistent RUQ pain, fever, and a positive Murphy’s sign (4).
Role of POCUS in Diagnosing Biliary Complications
POCUS utilizes a curvilinear transducer (3–5 MHz) for hepatobiliary imaging. The probe is positioned in the RUQ, using the liver as an acoustic window to visualize the gallbladder, bile ducts, and surrounding structures. Sonographic findings are interpreted based on established criteria (5).
Key Features of Biliary Colic
- Gallstones: Hyperechoic structures with posterior acoustic shadowing, often seen in the gallbladder lumen.
- Normal Gallbladder Wall Thickness: Less than 3 mm is typical in biliary colic, without signs of inflammation (6).
- Absence of Pericholecystic Fluid: This differentiates biliary colic from cholecystitis.
Key Features of Acute Cholecystitis
- Gallbladder Wall Thickening: Wall thickness >3 mm indicates inflammation.
- Pericholecystic Fluid: Hypoechoic fluid around the gallbladder suggests advanced cholecystitis or impending rupture.
- Sonographic Murphy’s Sign: Pain elicited during transducer compression over the gallbladder correlates with inflammation (1).
Accuracy and Sensitivity
Multiple studies demonstrate that POCUS has a sensitivity of 87% and specificity of 82% for diagnosing acute cholecystitis, comparable to formal radiologic imaging when performed by trained operators (2,4).
Advantages of POCUS in Biliary Diagnostics
- Timeliness: POCUS facilitates immediate diagnosis, enabling quicker treatment initiation, particularly in resource-limited settings.
- Portability: Its bedside application reduces the need for patient transportation to radiology, a critical factor in unstable patients.
- Cost-Efficiency: By minimizing reliance on advanced imaging modalities, POCUS reduces healthcare costs.
- Enhanced Patient Safety: Avoiding radiation exposure makes POCUS particularly advantageous in pregnant or pediatric populations (6).
Limitations of POCUS
Despite its benefits, POCUS is operator-dependent, requiring significant training and expertise. Suboptimal visualization due to obesity, bowel gas, or anatomical variations can reduce diagnostic accuracy. Additionally, complications such as gangrenous or emphysematous cholecystitis may necessitate further imaging (5).
Practical Guidelines for POCUS in Biliary Evaluation
- Patient Preparation: Position the patient in supine or left lateral decubitus to optimize RUQ imaging.
- Transducer Selection: Use a curvilinear probe with low frequency for deeper penetration.
- Scanning Technique: Identify the gallbladder in longitudinal and transverse planes. Assess for gallstones, wall thickness, and pericholecystic fluid. Perform a Murphy’s sign by applying gentle pressure with the transducer.
- Documentation: Save representative images or videos of abnormal findings for clinical records (1).
Conclusion
POCUS has transformed the management of biliary colic and acute cholecystitis, providing clinicians with a rapid, accurate, and non-invasive diagnostic tool. While challenges such as operator dependency persist, ongoing training and technological innovations are mitigating these limitations. As the adoption of POCUS continues to grow, its role in hepatobiliary imaging is set to become increasingly integral.
References
- Gaspari, R. J., et al. (2019). Emergency Ultrasound of the Abdomen and Pelvis: A Case-Based Approach. Cambridge University Press.
- Wong, J. M., et al. (2020). “Advances in the use of point-of-care ultrasound for hepatobiliary evaluation.” Critical Care Clinics, 36(4), 713-725.
- Lee, J., et al. (2018). “Point-of-care ultrasound in diagnosing gallbladder diseases: A review.” Journal of Clinical Ultrasound, 46(6), 334-342.
- Kirkpatrick, A. W., & Bree, A. (2017). Acute Care Ultrasound: Principles and Practice. CRC Press.
- Knight, R., et al. (2021). Ultrasound in Emergency Medicine. Wiley-Blackwell.
- Dietrich, C. F., et al. (2017). Ultrasound of the Gastrointestinal Tract. Springer.



















