A 70-year-old male with PMH of HTN, DM Type II and ongoing tobacco use presented with complaints of worsening DOE, orthopnea, weight gain and LE edema. He has been compliant with his Metoprolol, Basal-bolus Insulin regimen and ASA. He reports difficulty in completing routine tasks such as mowing his lawn and walking to his mailbox. Spouse reports that he has started sleeping in a recliner in the living room over the past 1 month. She also believes his abdominal girth has increased. He denies chest pain or pressure.
Family history of ischemic heart disease, CVA.
Temp – 98.4 degrees Fahrenheit
HR – 57 BPM
BP – 137/84 mm Hg
RR – 20 per minute
EKG shows – Q waves in inferior and lateral leads. No ST-T changes.
Physical exam is remarkable for JVD, rales / crackles in lung bases, 2+ pitting edema up to the upper thigh, abdominal distention with dullness to percussion in the flanks.
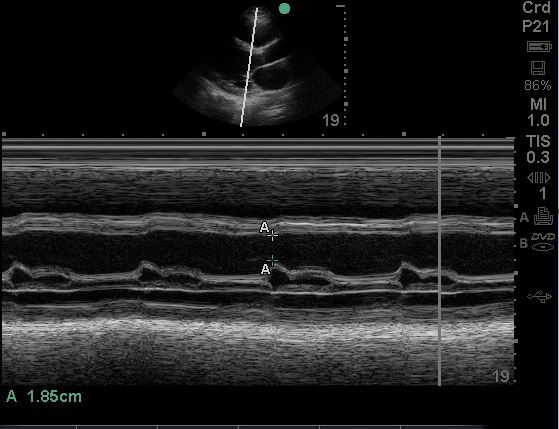
A POCUS cardiac exam was performed. Here is one of the videos from the patient’s echo. An M-mode tracing is also provided.
Question:
Is there any pathology seen?
A. Is the EF normal?
B. What is the approximate EF based upon the eyeball method of EF estimation?
Access the full POCUS Learning Library for FREE!
Share a few details so we can tailor new content to your specialty and region.



















