A 65-year-old male patient presented to the clinic for a routine physical exam. He is a known smoker. He had PMH of HTN, DM Type II and ongoing tobacco use. He did not complain of chest pain or dyspnea. The patient does complain of mild discomfort and pain in the lower abdomen, increased frequency of urination and occasional blood in the urine. He does not have any episode of passing gravel in the urine.
There is a family history of ischemic heart disease, CVA.
Temp – 98.4 degrees Fahrenheit, HR – 68 BPM, BP – 140/90 mm Hg, RR – 22 per minute
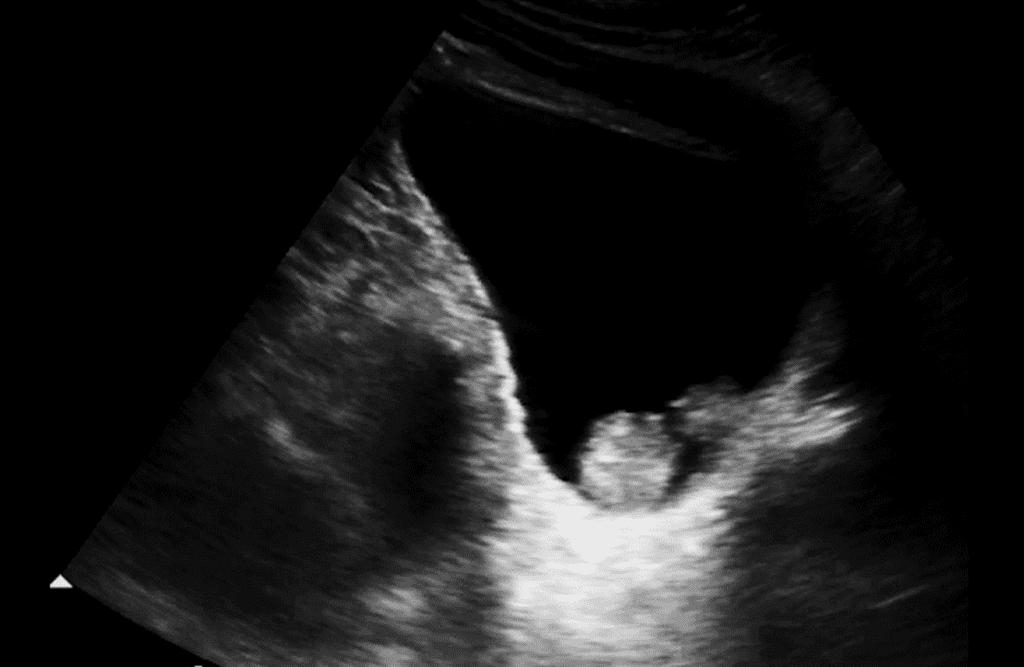
There was no other significant finding. The patient was concerned that he may have BPH. A POCUS exam was performed to examine the kidneys, ureters and bladder. The kidneys were of normal length and echotexture and showed no evidence of a mass, calculus or hydronephrosis. The bladder scan was performed as well, and the following is the longitudinal image of the bladder. The echogenic lesion inside the bladder did not move when the patient was rolled to the left and right lateral decubitus position.
What is the most likely diagnosis?
A. BPH with enlarged median lobe protruding into the lumen of the bladder.
B. Bladder calculus
C. Normal bladder with focal contraction of detrusor muscle
D. Bladder mass – possible bladder carcinoma
The most likely diagnosis is bladder mass – possible bladder carcinoma.
Explanation
The image shows a well-defined hyperechoic mass attached to the bladder wall (mass did not move when the patient was rolled over in the lateral decubitus position – this may help differentiate it from a calculus) and protruding into the lumen of the bladder. Ultrasound cannot determine if a mass is cancerous. Small or flat tumors may be missed, and ultrasound is less sensitive for detecting very small lesions. The sensitivity of ultrasound for detecting bladder tumors is high (over 90%), but it is not perfect, especially for small or early lesions. Further evaluation is essential.
The gold standard for diagnosis is cystoscopy, a procedure where a thin camera is inserted into the bladder to directly visualize the mass and obtain a biopsy if needed. Additional imaging (CT or MRI) may be performed to better characterize the mass and assess for spread if cancer is suspected. The final diagnosis (benign vs. malignant) is made by examining tissue from a biopsy under a microscope. There is no evidence of BPH in the image. Bladder calculus may be mobile and have a posterior acoustic shadow and may also elicit Twinkling artifact with color Doppler. This does not appear to be focal contraction of the muscle. So, the best answer choice is “Bladder mass – possible bladder carcinoma”.
Interested in proving your expertise in Genitourinary/Renal POCUS? Check out our Genitourinary/Renal POCUS Certificate here.
Access the full POCUS Learning Library for FREE!
Share a few details so we can tailor new content to your specialty and region.



















