
Case Study:
A 35-year-old male with PMH of DM Type II and ongoing tobacco use presented to the emergency medicine department with complaint of dyspnea, palpitations and chest pain following a road traffic accident 3 hours ago.
The patient also has a family history of ischemic heart disease, CVA.
Temp – 98.2 degrees Fahrenheit, HR – 110 BPM, BP – 90/72 mm Hg, RR – 32 per minute
EKG – Normal but shows tachycardia.
Physical exam shows evidence of bruising on the anterior chest bilaterally.
The following tracing of the IVC was obtained using M-mode by the emergency medicine fellow. The IVC diameter was 0.26 cm during inspiration and 0.77 cm during expiration. Based upon the IVC observation and the history and physical findings, what is the most accurate statement regarding the patient’s hemodynamic state.
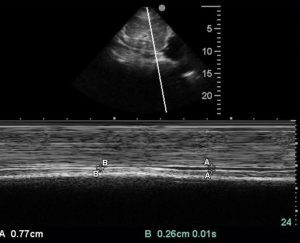
- The patient’s maximum IVC diameter suggests volume overload.
- The patient’s maximum IVC diameter and minimum diameter suggests euvolemic status.
- The IVC diameters suggest hypovolemic state but this patient is unlikely to benefit from intravenous fluid therapy.
- The maximum and minimum IVC diameter suggest hypovolemia and a responsive IVC. This patient would benefit from intravenous fluid therapy.
Answer: 4
Explanation:
A quick view of the IVC in the mid longitudinal plane gives a fairly good idea of the volume status is most clinical scenarios. Keep in mind that IVC diameter is just a number and there could be exceptions. It is important to acquire the measurement in the correct plane and at approximately 2.0 cm from the inferior cavoatrial junction (junction of IVC and the right atrium) and correlate it clinically.
Even though the maximum and minimum IVC can be measured using two separate images obtained with B-mode images, it is more convenient and probably more accurate using M-mode. While performing the scan the patient should be in the supine position. The patient should be breathing normally and told not to stop breathing. The variation in the IVC diameter is caused by the negative intrathoracic pressure during inspiration leading to increased RV filling and thus we get the reduction in IVC diameter during inspiration in normal patients. If the patient is volume overloaded or CVP is markedly elevated, then there could be reduced decrease in diameter or even no change in severe cases of volume overload.
The extreme ends of the IVC diameter measurements are more important and the variation with respiration is also equally important. For example, a well conditional super athlete may have a normal maximum IVC diameter of more than 3.0 cm. This in an average individual may represent volume overload or markedly elevated CVP. However, it may be normal in the athletic individual provided the IVC collapses 50% or more in those individuals with deep inspiration. See the chart below to get an approximate correlation of the CVP with the corresponding IVC diameter and its percentage collapse with inspiration.
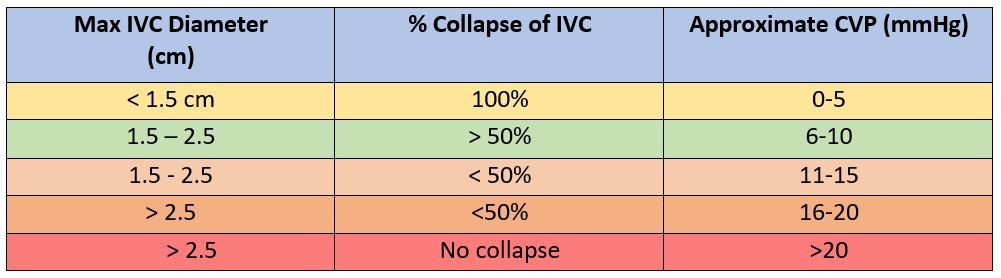
In the clinical scenario presented in the case, the maximum IVC diameter is less than 1.5 cm. So, the patient is hypovolemic and has low CVP. Since the IVC collapsed >50% on inspiration, this patient should benefit from intravenous fluid therapy.
_____
Interested in going further in your expertise in Abdominal Trauma? Check out our Abdominal Trauma Certificate here.



















