By Victor V Rao MBBS, DMRD, RDMS
Introduction
Lung point-of-care ultrasound (POCUS) and cardiac POCUS can help distinguish chronic obstructive pulmonary disease (COPD) exacerbation from acute decompensated heart failure (ADHF) in dyspneic patients with overlapping clinical presentations, especially when integrated with BNP and CXR rather than used in isolation.
Ultrasound has been a gamechanger in the diagnosis and management of the above-mentioned clinical conditions and can help you save the life of your patients with correct diagnosis and appropriate timely management.
Pathophysiologic Ultrasound Phenotypes
In acute COPD exacerbation without concomitant HF, the lung is typically “dry”, reflecting hyperinflation and airway inflammation rather than interstitial and or alveolar flooding. On lung ultrasound we will observe normal lung sliding with a predominant A-line pattern, few (< 3) or no B-lines, and often diaphragmatic flattening and increased excursion effort.
In contrast, ADHF will show evidence of hydrostatic pulmonary edema with interstitial and or alveolar fluid causing diffuse vertical artifacts (B-lines > 3) and often pleural effusions plus elevated filling pressures on focused echo and IVC assessment.

Figure 1. A-line pattern in lung ultrasound. A-lines are horizontal, hyperechoic reverberation artifacts seen deep and parallel to the pleural line and are typical of aerated lungs. A-lines repeat at regular, equal intervals, each one about the same distance apart as skin-to-pleura depth and gradually fade with depth. Be aware that this could be a normal finding too. See figure 2.
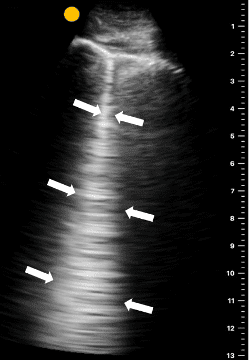
Figure 2. Single B-line seen in an intercostal space. This may be a normal finding and may not be clinically significant. B‑lines on lung ultrasound are vertical, hyperechoic, ring‑down artifacts arising from the pleural line that extend all the way to the bottom of the ultrasound screen without fading like A-lines, move with lung sliding, and erase A‑lines, suggestive of increased lung interstitial or alveolar fluid or fibrosis. A small number of B‑lines (usually < 3 per field of view) can be seen in some normal individuals, especially elderly patients and at dependent lung bases, and may be physiologic. 3 or more B‑lines in a single intercostal space, especially when seen in multiple zones bilaterally, in acute dyspnea suggests interstitial syndrome such as pulmonary edema as in ADHF. See figure 3.
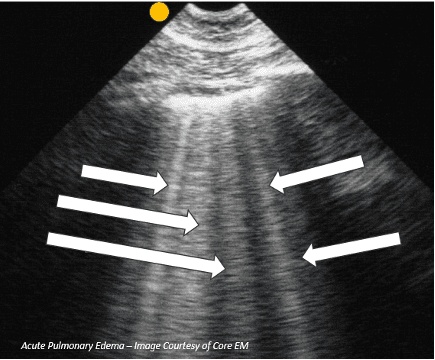
Figure 3. Multiple B-lines in a patient with acute pulmonary edema.
Lung Ultrasound Patterns: COPD vs CHF
Recent COPD cohorts show that quantification of B-lines can unmask concurrent HF during acute exacerbation of chronic obstructive pulmonary disease (AECOPD). In a 2024 multicenter study of ED patients with AECOPD, a lung ultrasound score based on B-line counts (LUS score >15) identified a cardiac origin of dyspnea with good diagnostic performance against a reference combining exam, NT proBNP, and echocardiography.
Contemporary data confirm that COPD alone is usually associated with a “dry lung” pattern, so even the absence of B-lines supports exclusion of pulmonary congestion in dyspneic COPD patients. Conversely, multiple bilateral B-lines (e.g., ≥3 per interspace in ≥2 zones per hemithorax) and higher global B-line scores correlate with heart failure (HF) severity and adverse outcomes in acute HF populations.
Pleural line morphology and distribution also help, cardiogenic edema produces relatively homogeneous, symmetric B-lines starting in dependent zones, whereas focal, asymmetric B-lines with irregular pleura favor pneumonia or ARDS over pure ADHF. In a COPD exacerbation, pleural effusions are uncommon. The presence of pleural effusion, especially bilateral and anechoic, should raise suspicion for HF.
Combined Heart–Lung POCUS Approach
Integrated heart–lung POCUS has shown high diagnostic accuracy and shorter time-to-diagnosis for undifferentiated dyspnea. A 2025 prospective ED study (61 dyspneic patients) reported that combined heart–lung ultrasound achieved 95% overall diagnostic accuracy for the final ED diagnosis, with sensitivity 98% and specificity 90% for HF, substantially improving early etiologic classification.
Another recent dyspnea cohort found lung ultrasound’s sensitivity and NPV for ruling out acute HF were comparable or superior to CXR and NT proBNP, while results were available in a median of 10 minutes vs more than an hour for radiography.
In practice, cardiopulmonary POCUS for “COPD vs CHF” depends on three findings.
1. Lung: A-line–predominant, “dry” pattern suggests COPD; diffuse B-lines (especially with pleural effusions) supports HF or mixed pathology.
2. Cardiac: Reduced LV systolic function, dilated LV, or markedly enlarged LA, plus mitral inflow/annular Doppler when available, support HF; a relatively normal LV with signs of pulmonary hypertension/right heart strain may align more with advanced COPD.
3. IVC: Dilated IVC with minimal respiratory variation suggests elevated right atrial pressure typical of volume overload while a small, collapsible IVC better fits isolated COPD exacerbation or hypovolemia.
A Practical Bedside Algorithm
Based on recent ED and hospitalist literature, a pragmatic POCUS-first sequence for a wheezing, tachypneic, undifferentiated patient would be:
1. Lung ultrasound (8–12 zones)
- Predominantly A-lines, preserved sliding, no effusions would strongly support COPD exacerbation. Do consider alternative non-cardiogenic causes if clinically discordant.
- Bilateral, relatively symmetric B-lines with or without pleural effusions suggest ADHF or mixed COPD/HF. Quantify B-lines to risk-stratify and monitor decongestion.
2. Focused cardiac views
- Depressed LV function, enlarged LA, secondary functional MR, or global hypokinesis reinforce HF diagnosis. POCUS can be performed by non-cardiologists with appropriate training and has been incorporated into hospitalist and ED quality-improvement programs.
- Isolated RV enlargement, septal flattening, and elevated RVSP in a lung “dry” pattern point toward COPD with pulmonary hypertension rather than primarily left-sided failure.
3. IVC assessment and integration with BNP/CXR
- Dilated non-collapsing IVC plus B-lines and LV dysfunction is highly consistent with ADHF.
- Normal or collapsible IVC in an A-line pattern and hyperinflated lungs supports COPD exacerbation even in the presence of nonspecific chest radiography.
See the flowchart below to help differentiate COPD exacerbation versus ADHF in a patient presenting with dyspnea. Be aware that in some patients a more complex picture may be present. Always correlate clinically.

Figure 4. Flowchart showing a simple practical POCUS algorithm to assess a patient with dyspnea with unclear COPD versus ADHF.
Key Differentiating Ultrasound Features
| Bedside Feature | Typical AECOPD | Typical ADHF Pulmonary Edema |
| Lung pattern | Predominant A-lines, normal sliding, “dry lung” in most cases. | Multiple bilateral B-lines, often diffuse and gravity dependent. |
| Pleural effusion | Usually absent or small if present. | Frequent; bilateral, anechoic or mildly complex. |
| LV function on POCUS | Often normal or mildly impaired; may see RV enlargement/pulmonary hypertension instead. | Frequently reduced EF or significant diastolic dysfunction. |
| IVC | Normal diameter, good inspiratory collapse (unless cor pulmonale/PH). | Dilated with reduced collapsibility, indicating high RA pressure. |
| B-line quantification | Low LUS score in isolated COPD; higher scores suggest occult HF in AECOPD. | Higher B-line burden correlates with hemodynamic congestion and worse outcomes. |
Table 1. Some key differentiating ultrasound features of a typical AECOPD versus typical ADHF pulmonary edema
Collectively, recent peer reviewed data and contemporary cardiopulmonary POCUS programs support using a structured lung–heart–IVC protocol to distinguish COPD exacerbation from ADHF at the bedside, recognizing that mixed phenotypes are common and that B-line quantification in AECOPD can identify the subset with clinically significant concomitant HF.
Key Ultrasound Findings in HF
- B-lines
- Vertical, laser-like hyperechoic artifacts arising from the pleural line, extending to the bottom of the screen without fading, and moving with lung sliding.
- Represent alveolar–interstitial syndrome and correlate with extravascular lung water; multiple studies link B-line burden to pulmonary congestion severity and HF outcomes.
- In acute HF, you typically see bilateral, relatively symmetric, and diffuse B-lines (B-profile), often from multiple intercostal spaces and lung zones.
- Pleural line and distribution
- Pleural line often appears thickened and irregular when congestion coexists with interstitial inflammation, but in pure cardiogenic edema the pleural line may be relatively smooth.
- B-lines usually spare the very apices in mild congestion and progress to involve anterior and lateral zones as pulmonary edema worsens.
- Associated findings
- Small bilateral pleural effusions are common and strengthen a cardiogenic picture when paired with diffuse B-lines.
- When integrated with echo (reduced LV function, elevated filling pressures) and IVC plethora, diffuse B-lines substantially increase specificity for acute HF versus primary airway disease.
Key Ultrasound Findings in COPD
- A-lines
- Horizontal reverberation artifacts, equidistant from each other and the pleural line, reflecting high air content beneath the pleura.
- Typical COPD/asthma pattern in acute exacerbation is an A-profile: normal lung sliding, predominant A-lines, and absence of diffuse B-lines in anterior fields.
- This A-profile with preserved sliding, especially when posterior fields are also A-line–dominant and no PLAPS (posterolateral alveolar/pleural syndrome) is present, strongly points toward non-parenchymal causes of dyspnea such as COPD/asthma or pulmonary embolism.
- Pleural line and distribution
- Pleural line in COPD may appear normal or mildly irregular but without the dense vertical artifacts seen in interstitial edema.
- Hyperinflation may reduce acoustic windows; you still mainly see A-lines and lung sliding, sometimes with reduced diaphragmatic excursion on subcostal views.
- Normal lung artifact pattern in a sick patient
- In a patient with significant dyspnea, a largely normal-appearing LUS (A-profile, sliding present, no or minimal B-lines, no effusion, no consolidation) is itself a clue favoring obstructive airway disease, PE, or non-pulmonary causes over HF-related pulmonary edema.
Final Thoughts
- Heart failure (cardiogenic pulmonary edema)
- Dominant artifact: multiple, diffuse B-lines (B-profile), often bilateral and symmetric.
- Typical add-ons: small bilateral effusions, possibly mildly thickened pleura and supportive cardiac/IVC findings.
- Clinical correlation: acute/subacute dyspnea, orthopnea, elevated BNP, JVD, peripheral edema.
- COPD/asthma exacerbation
- Dominant artifact: A-profile (A-lines with preserved lung sliding), often across anterior and lateral fields, with no diffuse B-lines and no PLAPS.
- Typical add-ons: hyperinflation signs (low, flattened diaphragm; reduced excursion) and otherwise “dry” lungs on ultrasound; cardiac filling may be reduced rather than overloaded.
- Clinical correlation: expiratory wheeze, history of COPD/asthma, hyperinflation on prior imaging, no orthopnea or overt volume overload.
Remember that COPD and HF may often coexist. Up to one‑third of “COPD exacerbations” may have a significant HF contribution, so mixed patterns are common. Focal or patchy B-lines (for example – around dependent regions or coexisting pneumonia) can complicate interpretation, so integrating artifact patterns with distribution, pleural effusion findings, and basic cardiac views provides the most reliable differentiation.
POCUS outperforms isolated CXR and auscultation for detecting pulmonary edema and improves accuracy of ADHF diagnosis when combined with clinical assessment. It is my hope that all POCUS users will integrate POCUS in the diagnosis and management of COPD and HF.
References
- Value of Lung Ultrasound Sonography B-Lines Quantification as a Marker of Heart Failure in COPD Exacerbation Fadwa Lajili et al. Int J Chron Obstruct Pulmon Dis. 2024 Aug 1; 19:1767–1774. doi: 10.2147/COPD.S447819
- Lung Ultrasound to Assess Pulmonary Congestion in Patients with Acute Exacerbation of COPD – Int J Chron Obstruct Pulmon Dis. 2023 Apr 25; 18:693–703. doi: 10.2147/COPD.S396855 PMCID: PMC10148645 PMID: 37128214
- Lung Ultrasound Offers Fast and Reliable Exclusion of Heart Failure in the Emergency Department: A Prospective Diagnostic Study Adis Keranović et al. 2025 Dec 6;15(24):3100. doi: 10.3390/diagnostics15243100 PMCID: PMC12731969 PMID: 41464101
- Quantification of residual pulmonary congestion defined by B-line findings on lung ultrasound to predict cardiovascular events in acute heart failure: A systematic review and meta-analysis Kevin Fernando Suhardi et al. doi: 10.1016/j.ihj.2025.05.003
- Three-view bedside ultrasound to differentiate acute decompensated heart failure from chronic obstructive pulmonary disease. doi: 10.1016/j.ajem.2012.11.028 PMID: 23380088
- Acute Pulmonary Edema – https://coreem.net/core/ape/
- Diagnostic value of combined heart and lung ultrasound in emergency department patients with dyspnea, Anna Bjällmark et.al., doi: 10.1111/cpf.70009 PMID: 40243381 PMCID: PMC12005122.
*Disclaimer
AI (Perplexity Pro) was used to conduct extensive research on this topic and draft the outline. The author has reviewed, verified and edited the content for accuracy and relevance to POCUS. Some views are the author’s own views but are based on consensus of the medical community.
Access the full POCUS Learning Library for FREE!
Share a few details so we can tailor new content to your specialty and region.



















