Written by Dr. Thushini Goonewardene
A 35-year-old young, healthy male, known to have dislocated his right shoulder once before, presents with right sided shoulder pain. He states that the onset of pain occurred after he tried to move a heavy object. He denied any direct trauma to his shoulder.
On examination, there is loss of normal contour of his right shoulder and the acromion appears prominent. A bulge is noted anteriorly, just inferior to the right coracoid process. His right upper limb is held supported by his left hand and all movements at the right shoulder joint are restricted. There are no neurovascular deficits noted.
Question 1
What is your clinical diagnosis?
Answer
Right anterior shoulder dislocation
Question 2
Does this patient require a radiograph prior to reduction?
Answer
A radiograph of the shoulder joint is performed to look for possible fractures which could either be a contraindication to a closed reduction in ED or may complicate the reduction process. It will also enable one to determine the type of dislocation; whether anterior, posterior or inferior, allowing to decide on the reduction technique.
However, using the Quebec decision rule for radiography in shoulder dislocation pre-reduction radiography may be avoided in anterior shoulder dislocations, if none of the four risk factors are present. The Quebec decision rule is a prospectively derived clinical decision rule, aimed at reducing the number of pre-and post-reduction films in anterior shoulder dislocation. The algorithm reached a sensitivity of 100%, specificity of 34.2% and a negative predictive value of 99.2% and is based on four at-risk factors:
- Age ≥40 years
- Mechanism (MVC, assault, sporting injury, fall from greater than patient’s height)
- Presence of humeral ecchymosis
- First episode of dislocation
This algorithm is projected to reduce the number of pre-reduction films by 28% and post-reduction films by 82%. It should be noted, however, all patients in the study had a GCS of 15 and that this clinical decision rule has yet to be validated.
POCUS is useful in such patients to differentiate between anterior and posterior dislocations as well as to confirm whether the reduction manoeuvre has been successful or not. Using POCUS has the added advantage of being able to perform at the bedside, before the procedural sedation wears off. This allows further reattempts at manipulation if required without the need for re-sedation.
Question 3
Name structures A, B, C, D, E on the image given below.
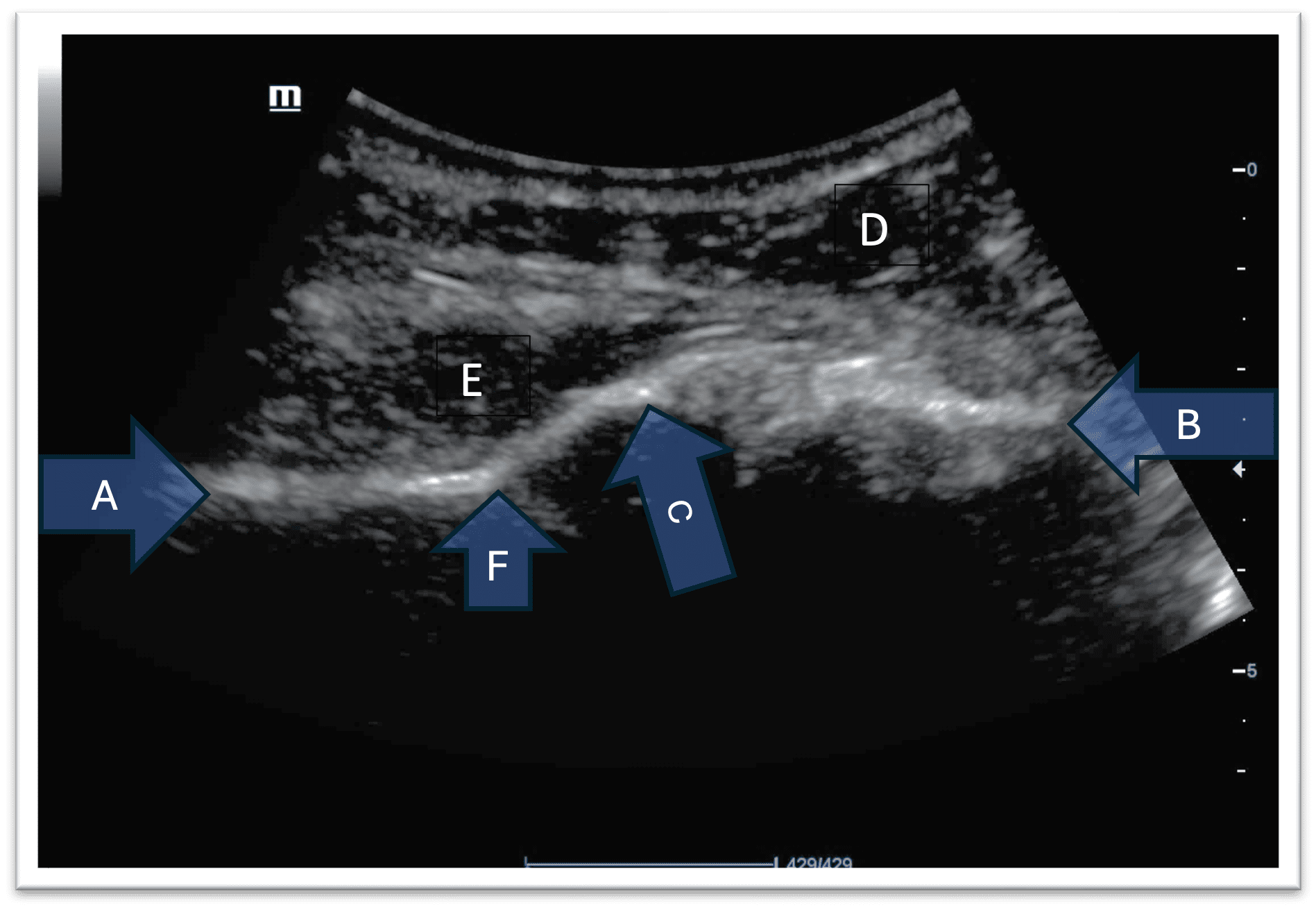
Figure 1. Ultrasound scan image of a normal right shoulder joint (posteriorly) The image left to right corresponds to the patient’s medial to lateral.
Answer
A – Body of scapula
B – Head of humerus
C – Glenoid
D – Deltoid muscle
E – Infraspinatus muscle
F – Spinoglenoid notch
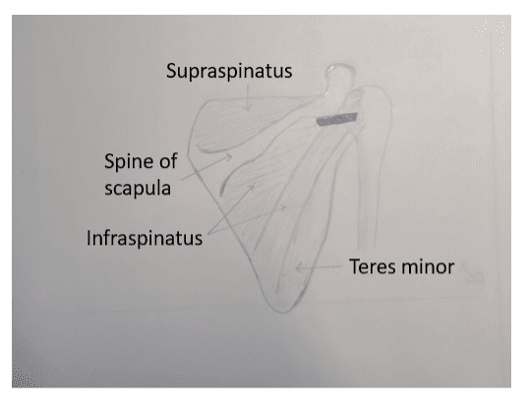
Figure 2. Position of probe across the posterior aspect of the shoulder joint
Question 4
What type of dislocation is this?
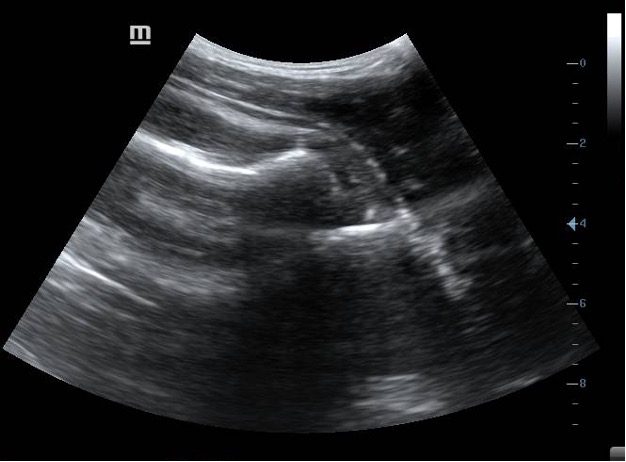
Figure 3. Ultrasound scan image of the right shoulder joint (posteriorly) The image left to right corresponds to the patient’s medial to lateral
Answer
Anterior
In a normal shoulder joint the head of the humerus will be located within the glenoid cavity. On ultrasound the glenoid rim and the head of the humerus will appear to lie in the same horizontal plane.
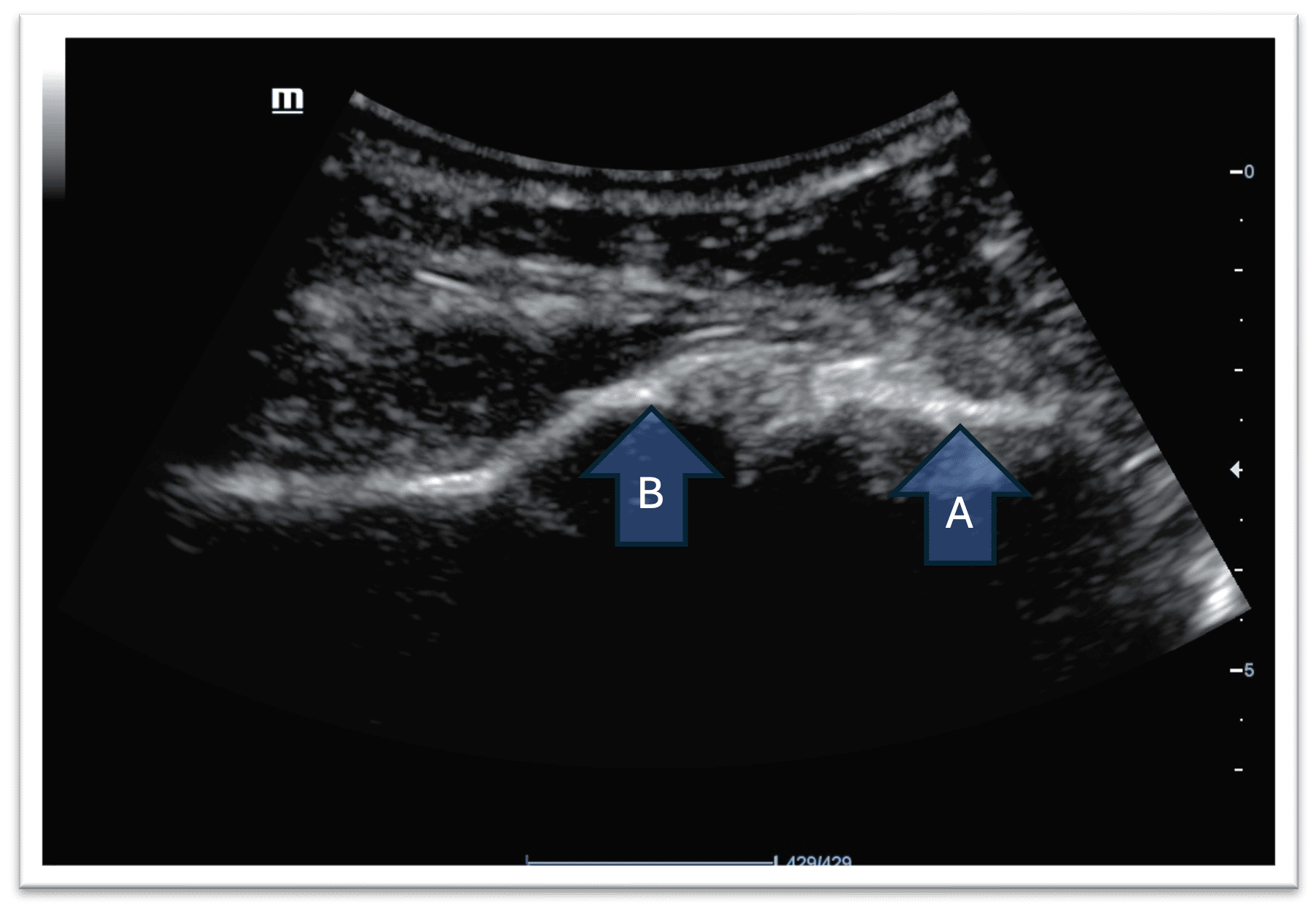
Figure 4. Normal Shoulder joint A – Head of humerus B – Glenoid
In this patient, the glenoid rim and the head of the humerus are not lying in the same horizontal plane. This indicates a dislocation.
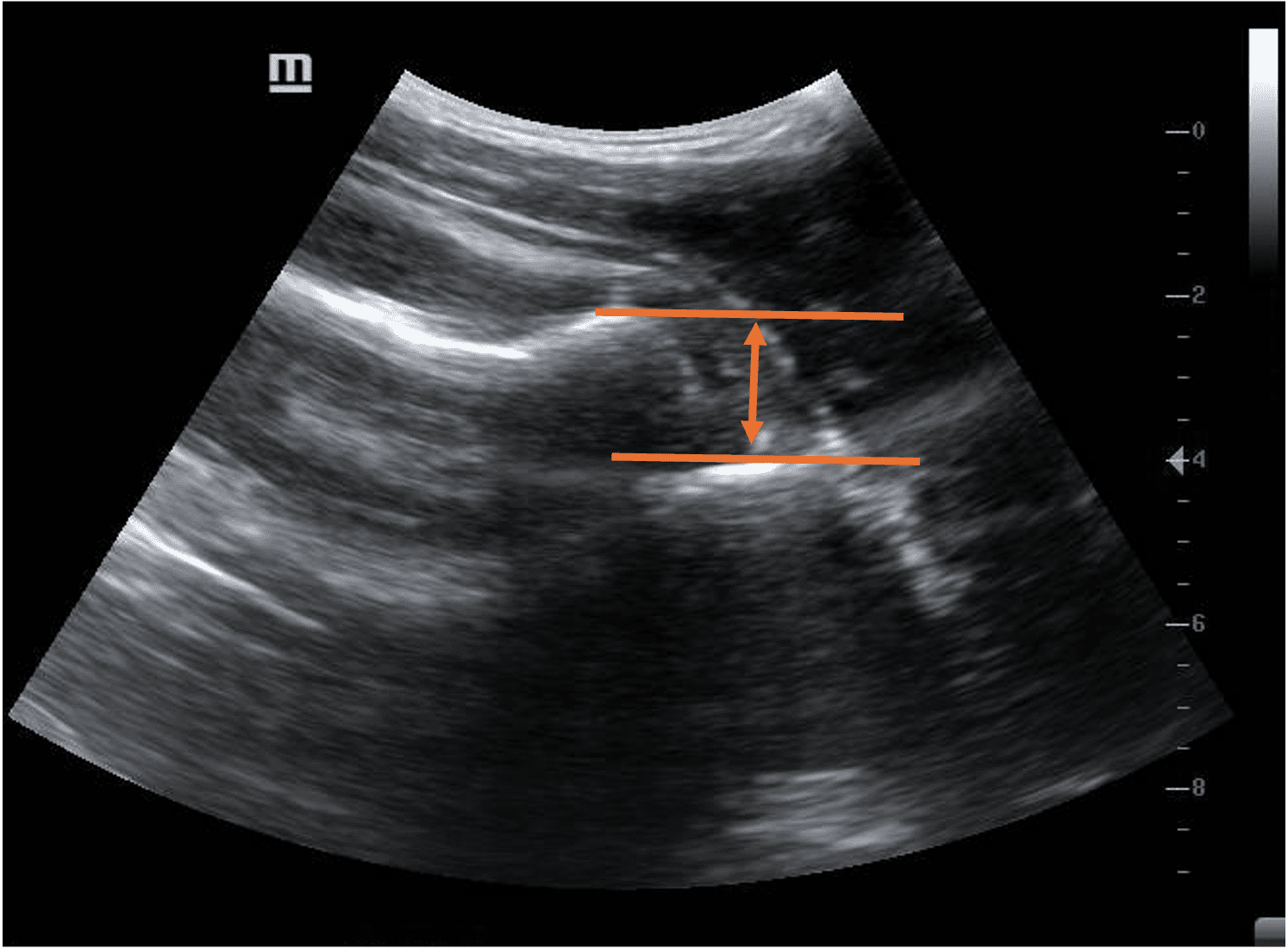
Figure 5. Anterior dislocation of the shoulder
Note how the head of the humerus is located deeper in the image. This means that the head of the humerus is located further away from the probe. This is an anterior dislocation of the shoulder joint.
In the event of a posterior shoulder dislocation, the head of the humerus will appear closer to the probe.
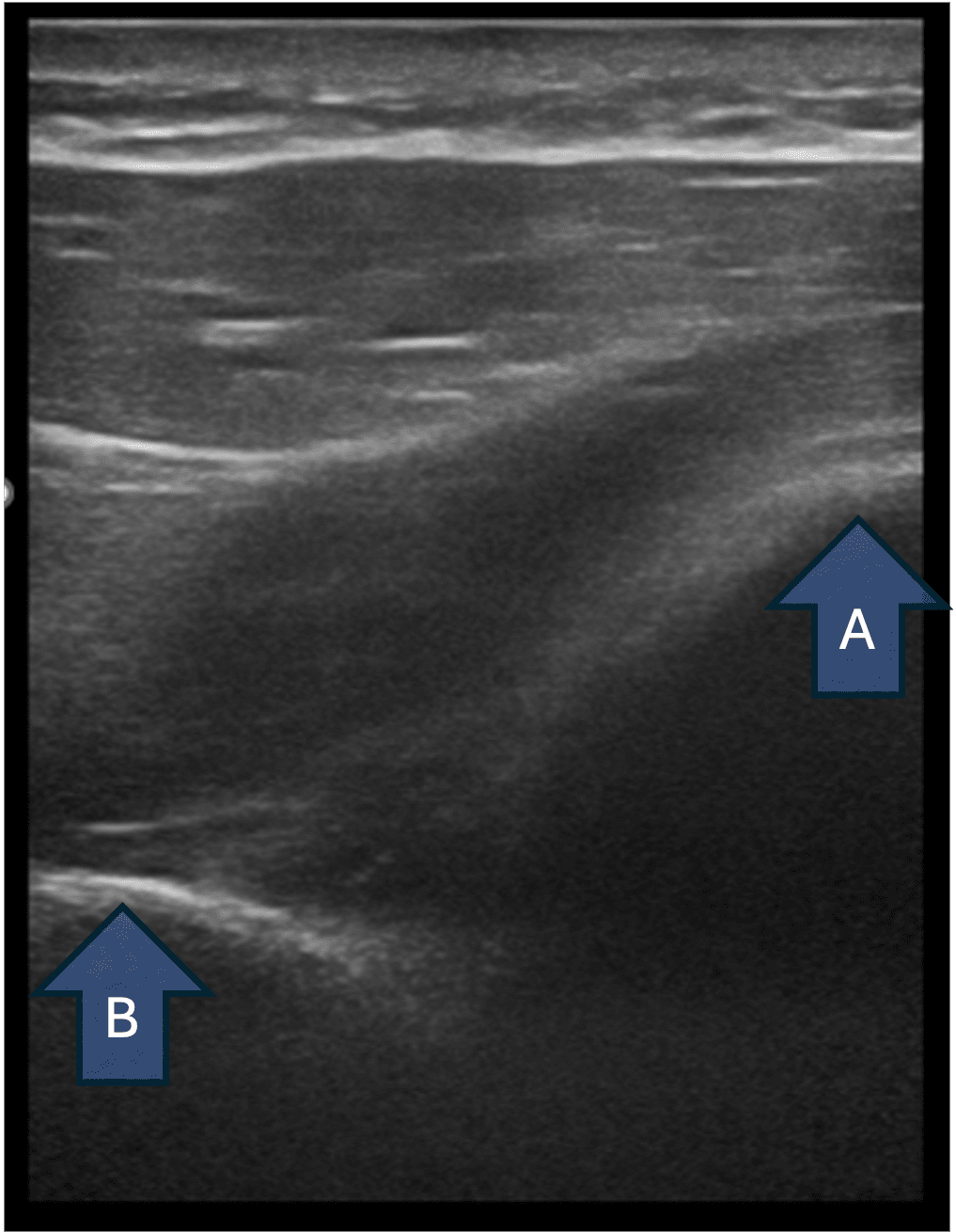
Figure 6. Posterior dislocation of the shoulder A- Head of humerus B- Glenoid
The patient’s shoulder joint was manipulated under procedural sedation using the Kocher’s method.
Question 5
Is the reduction successful?
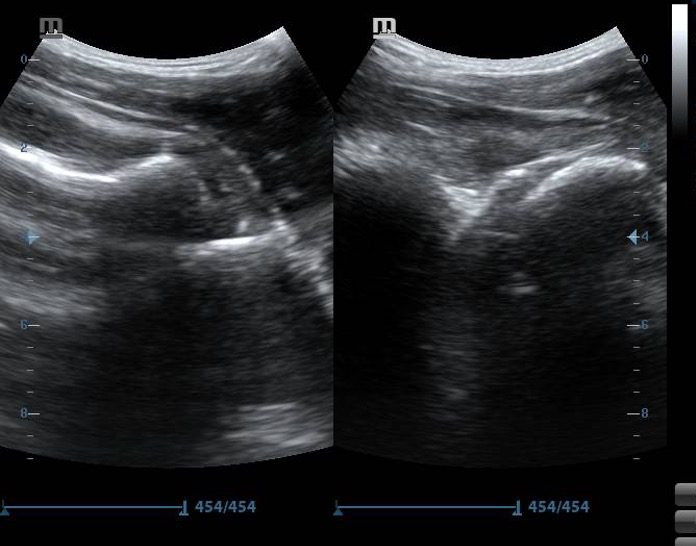
Figure 7. Pre-reduction (left) and post-reduction (right) images of right shoulder joint
Answer
Yes
The head of the humerus appears to be deeper in position compared to the glenoid rim on the first image. This indicates an anterior shoulder dislocation. The head of the humerus is in line with the glenoid rim in the image on the right, indicating successful reduction
Further confirmation of the reduction can be done by observing the head of the humerus on ultrasound while rotating the affected shoulder internally and externally with the arm adducted. The head will appear to move smoothly within the glenoid rim.
Learning points
- Use either a curvilinear or linear probe (with virtual convex setting, if available)
- Scan over the posterior aspect of the shoulder joint
- Place the probe in transverse orientation just below the spine of the scapula and move it laterally until you start to see the head of the humerus
- Attempt to move the arm (internal/ external rotation) this will help you locate the head of the humerus
- When the head of the humerus is positioned deep in the image – anterior dislocation
- When the head of the humerus is more superficially located – posterior dislocation
- Confirm success of your procedure by observing the smooth movement of the head of the humerus within the glenoid cavity with internal and external rotation of the adducted arm
- Drawbacks – Ultrasound can only be used to confirm anterior and posterior dislocations and not for inferior dislocations
References
- https://journalfeed.org/article-a-day/2020/msk-ultrasound-for-shoulder-dislocation/
- https://www.aliem.com/ultrasound-for-win-acute-shoulder-injury-us4tw/
- https://www.researchgate.net/publication/23937000_Refinement_of_the_Quebec_decision_rule_for_radiography_in_shoulder_dislocation



















