Case Study:
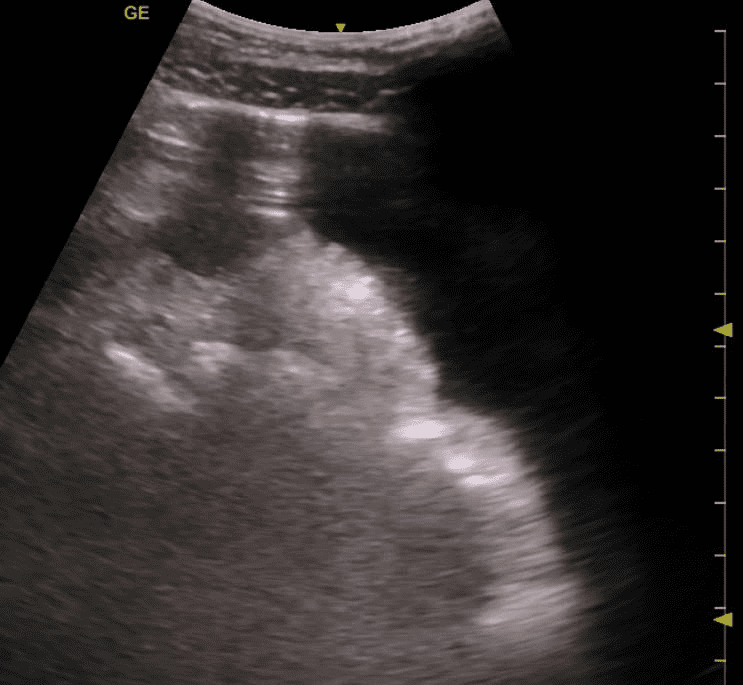
A 28-year-old male patient was brought to the emergency department with the chief complaint of fever, severe abdominal pain, and abdominal distension for the past 7 days. He took some antacids with no definite relief. He did give a history of travel to Haiti for a humanitarian project few weeks ago. There was no history of trauma. He had no significant past medical history and was not on any known medication. The patient claimed to be on a liquid diet for the past 5 days. On physical exam, the patient was lethargic, Temperature 102 Degrees F, BP 140/88 mmHg, SpO2 is 98% at room air. The abdomen seemed slightly distended with rebound tenderness. The ultrasound fellow decided to perform a quick POCUS abdomen exam. The following image was obtained by placing the transducer with the orientation marker pointing cephalad in the right upper quadrant close to the midline. The patient was scanned in the supine position.
- What is the most accurate diagnosis?
- Normal abdominal scan with bowel gas shadows.
- No free fluid seen in abdominal cavity.
- Bowel obstruction.
- Free fluid in abdominal cavity with abdominal a-lines (reverberation artifact) consistent with pneumoperitoneum.
Answer: 4 — Free fluid in abdominal cavity with abdominal a-lines (reverberation artifact) consistent with pneumoperitoneum.
Explanation:
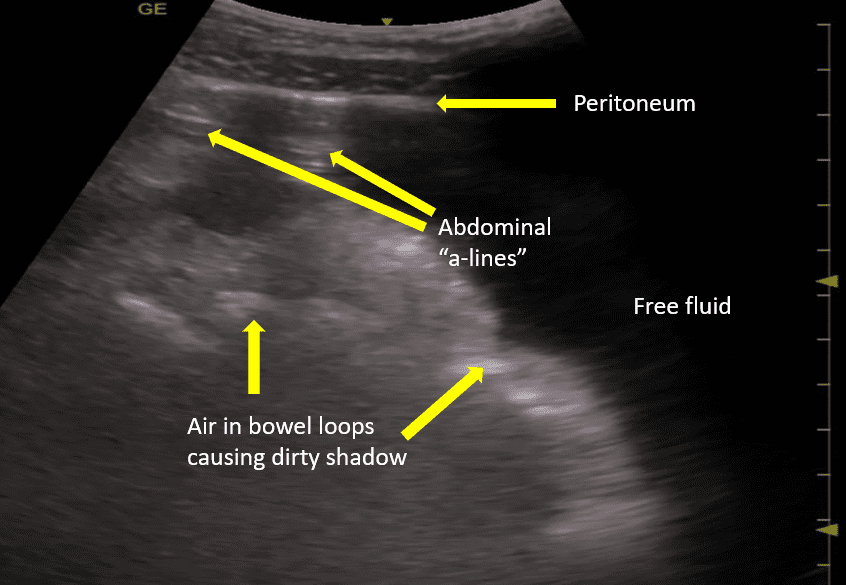
Large amount of anechoic free fluid is seen in the abdominal cavity with bowel loops floating in the fluid. The true nature of the free fluid can be accurately determined by performing an ultrasound guided paracentesis. Anteriorly, two reverberation artifacts are seen arising at the level of the parietal peritoneum. Since, air is lighter so it tends to rise above and with the patient in the supine position it can be seen sonographically as an abdominal “a-line” pattern (reverberation artifact) and it will move with change in patient position. Normally free air should not be seen inside the abdominal cavity unless a procedure was performed which could have introduced air into the peritoneal cavity or there is presence of gas forming organism infection. Air is normally seen with the bowel loops and it creates a “dirty shadow”. In this case the patient had Typhoid fever with perforation of the bowel. Exploratory laparotomy was performed, and the bowel perforation in the terminal ileum was surgically repaired. Fortunately, the patient recovered in 8 days and was discharged.
Reference:
https://link.springer.com/article/10.1007/s13089-011-0054-7
_____
Interested in going further in your expertise in Abdominal Trauma? Check out our Abdominal Trauma Certificate here.



















